

Unplanned readmission prevention by a geriatric emergency network for transitional care (URGENT): a prospective before-after study
- PMID: 31390994
- PMCID: PMC6686568
- DOI: 10.1186/s12877-019-1233-9
Unplanned readmission prevention by a geriatric emergency network for transitional care (URGENT): a prospective before-after study
Abstract
Background: URGENT is a comprehensive geriatric assessment (CGA) based nurse-led care model in the emergency department (ED) with geriatric follow-up after ED discharge aiming to prevent unplanned ED readmissions.
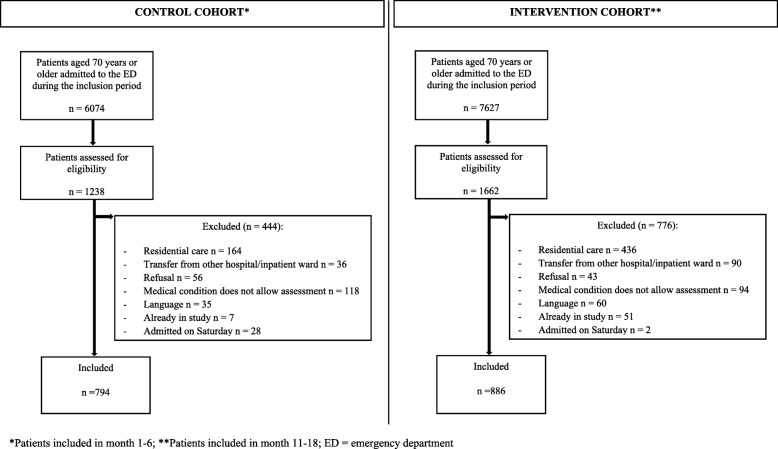
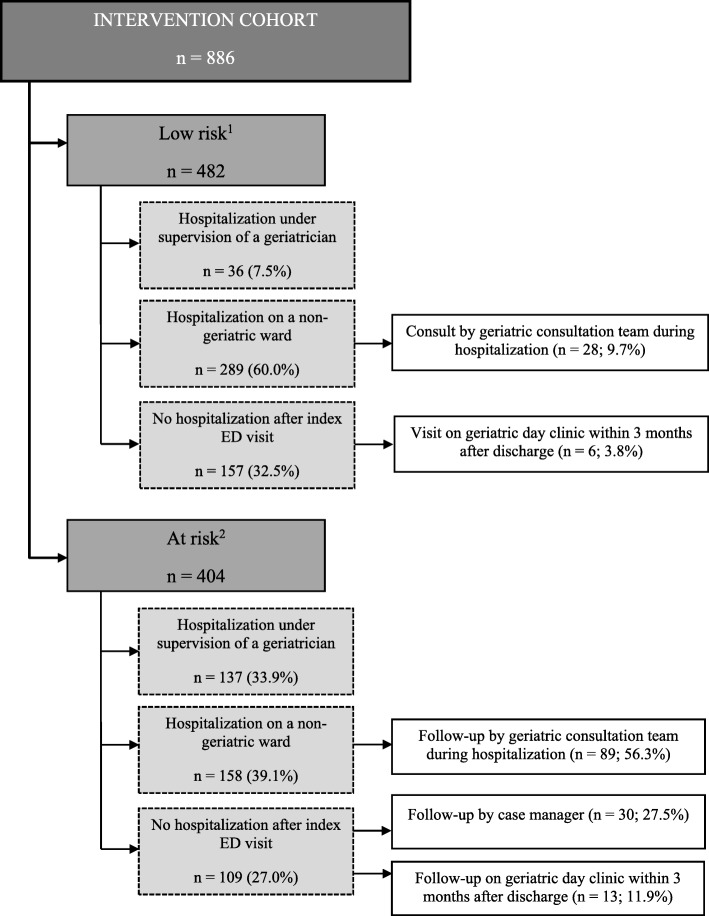
Methods: A quasi-experimental study (sequential design with two cohorts) was conducted in the ED of University Hospitals Leuven (Belgium). Dutch-speaking, community-dwelling ED patients aged 70 years or older were eligible for enrolment. Patients in the control cohort received usual care. Patient in the intervention cohort received the URGENT care model. A geriatric emergency nurse conducted CGA and interdisciplinary care planning among older patients identified as at risk for adverse events (e.g. unplanned ED readmission, functional decline) with the interRAI ED Screener© and clinical judgement of ED staff. Case manager follow-up was offered to at risk patients without hospitalization after index ED visit. For inpatients, geriatric follow-up was guaranteed on an acute geriatric ward or by the inpatient geriatric consultation team on a non-geriatric ward if considered necessary. Primary outcome was unplanned 90-day ED readmission. Secondary outcomes were ED length of stay (LOS), hospitalization rate, in-hospital LOS, 90-day higher level of care, 90-day functional decline and 90-day post-hospitalization mortality.
Results: Almost half of intervention patients (404/886 = 45.6%) were categorized at risk. These received on average seven advices. Adherence rate to advices on the ED, during hospitalization and in community care was 86.1, 74.6 and 34.1%, respectively. One out of four at risk patients without hospitalization after index ED visit accepted case manager follow-up. Unplanned ED readmission occurred in 170 of 768 (22.1%) control patients and in 205 of 857 (23.9%) intervention patients (p = .11). The intervention group had shorter ED LOS (12.7 h versus 19.1 h in the control group; p < .001), but higher rate of hospitalization (70.0% versus 67.0% in the control group; p = .003).
Conclusions: The URGENT care model shortened ED LOS and increased the hospitalization rate, but did not prevent unplanned ED readmissions. A geriatric emergency nurse could improve in-hospital patient management, but failed to introduce substantial out-hospital case-management.
Trial registration: The protocol of this study was registered retrospectively with ISRCTN ( ISRCTN91449949 ; registered 20 June 2017).
Keywords: Comprehensive geriatric assessment; Emergency department; Geriatric care model; Nurse-led; Unplanned ED readmission.
Conflict of interest statement
KM is a member of the editorial board of BMC Geriatrics (section editor). He was not involved in the editorial process of the current paper. All other authors declare that they have no competing interests.
Figures
References
-
- Kahn JH, Magauran BG, Jr, Olshaker SO. Geriatric emergency medicine: principles and practice. New York: Cambridge University Press; 2014.
-
- Deschodt M, Devriendt E, Sabbe M, Knockaert D, Deboutte P, Boonen S, et al. Characteristics of older adults admitted to the emergency department (ED) and their risk factors for ED readmission based on comprehensive geriatric assessment: a prospective cohort study. BMC Geriatr. 2015;15(1):54. doi: 10.1186/s12877-015-0055-7. - DOI - PMC - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
