

NA-CONTROL: a study protocol for a randomised controlled trial to compare specific outpatient rehabilitation that targets cerebral mechanisms through relearning motor control and uses self-management strategies to improve functional capability of the upper extremity, to usual care in patients with neuralgic amyotrophy
- PMID: 31391076
- PMCID: PMC6686223
- DOI: 10.1186/s13063-019-3556-4
NA-CONTROL: a study protocol for a randomised controlled trial to compare specific outpatient rehabilitation that targets cerebral mechanisms through relearning motor control and uses self-management strategies to improve functional capability of the upper extremity, to usual care in patients with neuralgic amyotrophy
Abstract
Background: Neuralgic amyotrophy (NA) is a distinct peripheral neurological disorder of the brachial plexus with a yearly incidence of 1/1000, which is characterised by acute severe upper extremity pain. Weakness of the stabilising shoulder muscles in the acute phase leads to compensatory strategies and abnormal motor control of the shoulder - scapular dyskinesia. Despite peripheral nerve recovery, scapular dyskinesia often persists, leading to debilitating residual complaints including pain and fatigue. Evidence suggests that persistent scapular dyskinesia in NA may result from maladaptive cerebral neuroplasticity, altering motor planning. Currently there is no proven effective causative treatment for the residual symptoms in NA. Moreover, the role of cerebral mechanisms in persistent scapular dyskinesia remains unclear.
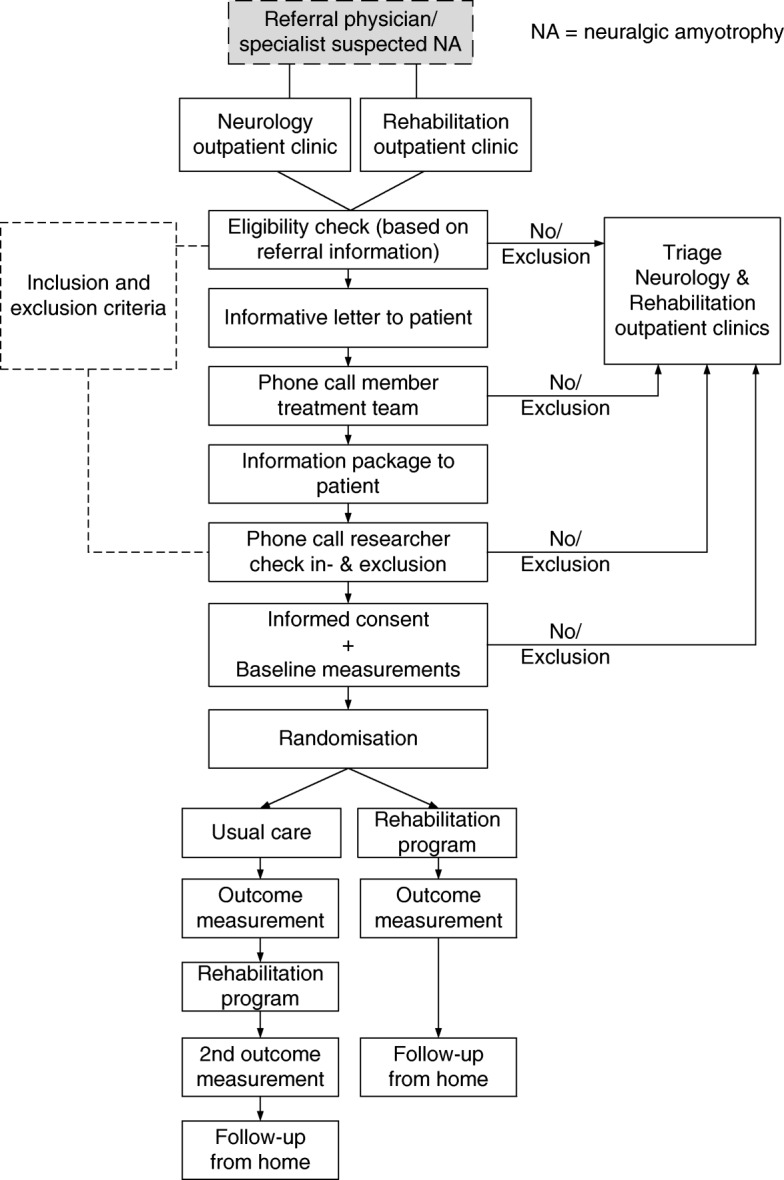
Methods: NA-CONTROL is a single-centre, randomised controlled trial comparing specific rehabilitation to usual care in NA. The rehabilitation programme combines relearning of motor control, targeting cerebral mechanisms, with self-management strategies. Fifty patients will be included. Patients are recruited through the Radboud university medical center Nijmegen, the Netherlands. Patients with a (suspected) diagnosis of NA, with lateralized symptoms and scapular dyskinesia in the right upper extremity, who are 18 years or older and not in the acute phase can be included. The primary outcome is the Shoulder Rating Questionnaire score, which measures functional capability of the upper extremity. Secondary clinical outcomes include measures of pain, fatigue, participation, reachable workspace, muscle strength and quality of life. In addition, motor planning is assessed with first-person motor imagery and functional magnetic resonance imaging. In a sub-study the patients are compared to 25 healthy participants, to determine the involvement of cerebral mechanisms. This will enable interpretation of cerebral changes associated with the rehabilitation programme and functional impairments in NA.
Discussion: NA-CONTROL is the first randomised trial to investigate the effect of specific rehabilitation on residual complaints in NA. It also is the first study into the cerebral mechanisms that might underlie persistent scapular dyskinesia in NA. It thus may aid the further development of mechanism-based interventions for disturbed motor control in NA and in other peripheral neurological disorders.
Trial registration: ClinicalTrials.gov, NCT03441347 . Registered on 20 February 2018.
Keywords: Maladaptive neuroplasticity; Motor control; Neuralgic amyotrophy; Neurorehabilitation; Occupational therapy; Parsonage Turner syndrome; Peripheral nerve dysfunction; Physical therapy; Scapular dyskinesia; Upper extremity.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures




References
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
