

Association between major surgical admissions and the cognitive trajectory: 19 year follow-up of Whitehall II cohort study
- PMID: 31391161
- PMCID: PMC6683971
- DOI: 10.1136/bmj.l4466
Association between major surgical admissions and the cognitive trajectory: 19 year follow-up of Whitehall II cohort study
Abstract
Objective: To quantify the association between major surgery and the age related cognitive trajectory.
Design: Prospective longitudinal cohort study.
Setting: United Kingdom.
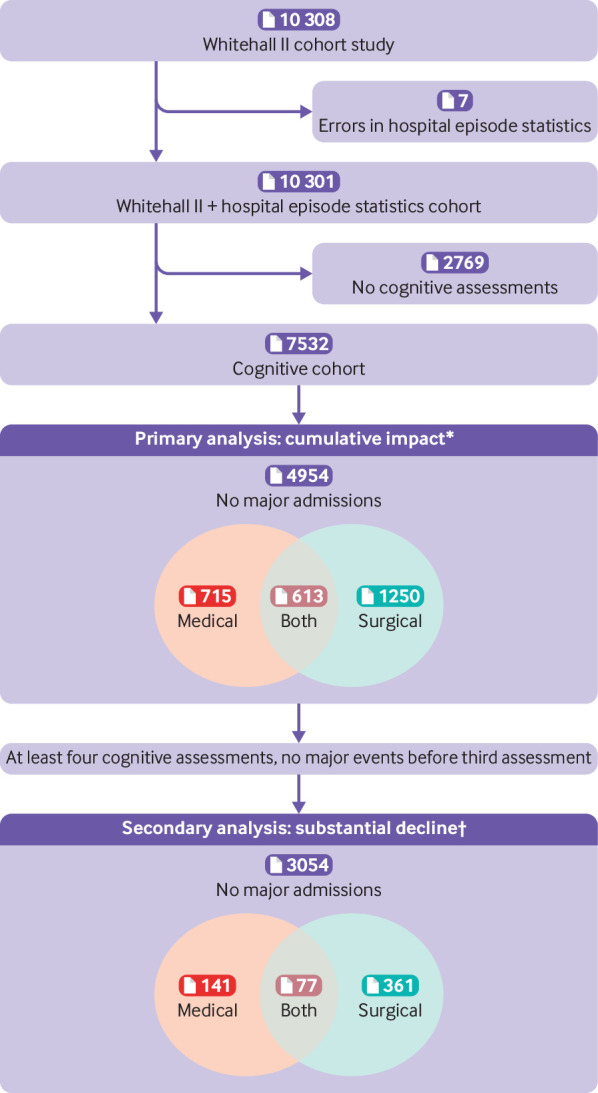
Participants: 7532 adults with as many as five cognitive assessments between 1997 and 2016 in the Whitehall II study, with linkage to hospital episode statistics. Exposures of interest included any major hospital admission, defined as requiring more than one overnight stay during follow-up.
Main outcomes measures: The primary outcome was the global cognitive score established from a battery of cognitive tests encompassing reasoning, memory, and phonemic and semantic fluency. Bayesian linear mixed effects models were used to calculate the change in the age related cognitive trajectory after hospital admission. The odds of substantial cognitive decline induced by surgery defined as more than 1.96 standard deviations from a predicted trajectory (based on the first three cognitive waves of data) was also calculated.
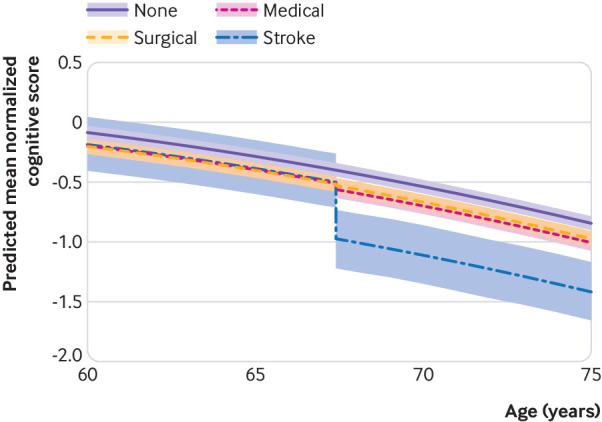
Results: After accounting for the age related cognitive trajectory, major surgery was associated with a small additional cognitive decline, equivalent on average to less than five months of aging (95% credible interval 0.01 to 0.73 years). In comparison, admissions for medical conditions and stroke were associated with 1.4 (1.0 to 1.8) and 13 (9.6 to 16) years of aging, respectively. Substantial cognitive decline occurred in 2.5% of participants with no admissions, 5.5% of surgical admissions, and 12.7% of medical admissions. Compared with participants with no major hospital admissions, those with surgical or medical events were more likely to have substantial decline from their predicted trajectory (surgical admissions odds ratio 2.3, 95% credible interval 1.4 to 3.9; medical admissions 6.2, 3.4 to 11.0).
Conclusions: Major surgery is associated with a small, long term change in the average cognitive trajectory that is less profound than for major medical admissions. The odds of substantial cognitive decline after surgery was about doubled, though lower than for medical admissions. During informed consent, this information should be weighed against the potential health benefits of surgery.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://group.bmj.com/group/rights-licensing/permissions.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf and declare: no support from any organisation for the submitted work ; no financial relationships with any organisations that might have an interest in the submitted work in the previous three years; no other relationships or activities that could appear to have influenced the submitted work.
Figures
Comment in
-
The determinants of cognitive decline and dementia.BMJ. 2019 Aug 7;366:l4946. doi: 10.1136/bmj.l4946. BMJ. 2019. PMID: 31391159 No abstract available.
-
Prolong the use of oxygen following surgery to improve cognitive trajectory.BMJ. 2019 Sep 12;366:l5483. doi: 10.1136/bmj.l5483. BMJ. 2019. PMID: 31515262 No abstract available.
-
Surgery and persistent cognitive decline: a commentary and an independent discussion.Br J Anaesth. 2020 Mar;124(3):229-234. doi: 10.1016/j.bja.2019.10.020. Epub 2019 Dec 12. Br J Anaesth. 2020. PMID: 31839254 No abstract available.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical