

A systematic review of comorbidities and outcomes of adult patients with pleural infection
- PMID: 31391221
- PMCID: PMC6860993
- DOI: 10.1183/13993003.00541-2019
A systematic review of comorbidities and outcomes of adult patients with pleural infection
Abstract
Background: Pleural infection remains an important cause of mortality. This study aimed to investigate worldwide patterns of pre-existing comorbidities and clinical outcomes of patients with pleural infection.
Methods: Studies reporting on adults with pleural infection between 2000 and 2017 were identified from a search of Embase and MEDLINE. Articles reporting exclusively on tuberculous, fungal or post-pneumonectomy infection were excluded. Two reviewers assessed 20 980 records for eligibility.
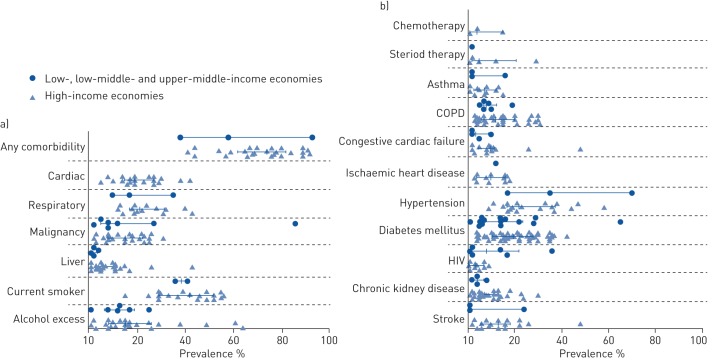
Results: 211 studies met the inclusion criteria. 134 articles (227 898 patients, mean age 52.8 years) reported comorbidity and/or outcome data. The majority of studies were retrospective observational cohorts (n=104, 78%) and the most common region of reporting was East Asia (n=33, 24%) followed by North America (n=27, 20%). 85 articles (50 756 patients) reported comorbidity. The median (interquartile range (IQR)) percentage prevalence of any comorbidity was 72% (58-83%), with respiratory illness (20%, 16-32%) and cardiac illness (19%, 15-27%) most commonly reported. 125 papers (192 298 patients) reported outcome data. The median (IQR) length of stay was 19 days (13-27 days) and median in-hospital or 30-day mortality was 4% (IQR 1-11%). In regions with high-income economies (n=100, 74%) patients were older (mean 56.5 versus 42.5 years, p<0.0001), but there were no significant differences in prevalence of pre-existing comorbidity nor in length of hospital stay or mortality.
Conclusion: Patients with pleural infection have high levels of comorbidity and long hospital stays. Most reported data are from high-income economy settings. Data from lower-income regions is needed to better understand regional trends and enable optimal resource provision going forward.
Copyright ©ERS 2019.
Conflict of interest statement
Conflict of interest: T.N. Cargill has nothing to disclose. Conflict of interest: M. Hassan has nothing to disclose. Conflict of interest: J.P. Corcoran has nothing to disclose. Conflict of interest: E. Harriss has nothing to disclose. Conflict of interest: R. Asciak has nothing to disclose. Conflict of interest: R.M. Mercer has nothing to disclose. Conflict of interest: D.J. McCracken has nothing to disclose. Conflict of interest: E.O. Bedawi has nothing to disclose. Conflict of interest: N.M. Rahman has nothing to disclose.
Figures


References
-
- Bedawi EO, Hassan M, Rahman NM. Recent developments in the management of pleural infection: a comprehensive review. Clin Respir J 2018; 12: 2309–2320. - PubMed
-
- Søgaard M, Nielsen RB, Nørgaard M, et al. . Incidence, length of stay, and prognosis of hospitalized patients with pleural empyema: a 15-year Danish nationwide cohort study. Chest 2014; 145: 189–192. - PubMed
-
- Shen H-N, Lu C-L, Li C-Y. Epidemiology of pleural infections in Taiwan from 1997 through 2008: pleural infections in Taiwan. Respirology 2012; 17: 1086–1093. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous