

Personalized circulating tumor DNA analysis to detect residual disease after neoadjuvant therapy in breast cancer
- PMID: 31391323
- PMCID: PMC7236617
- DOI: 10.1126/scitranslmed.aax7392
Personalized circulating tumor DNA analysis to detect residual disease after neoadjuvant therapy in breast cancer
Abstract
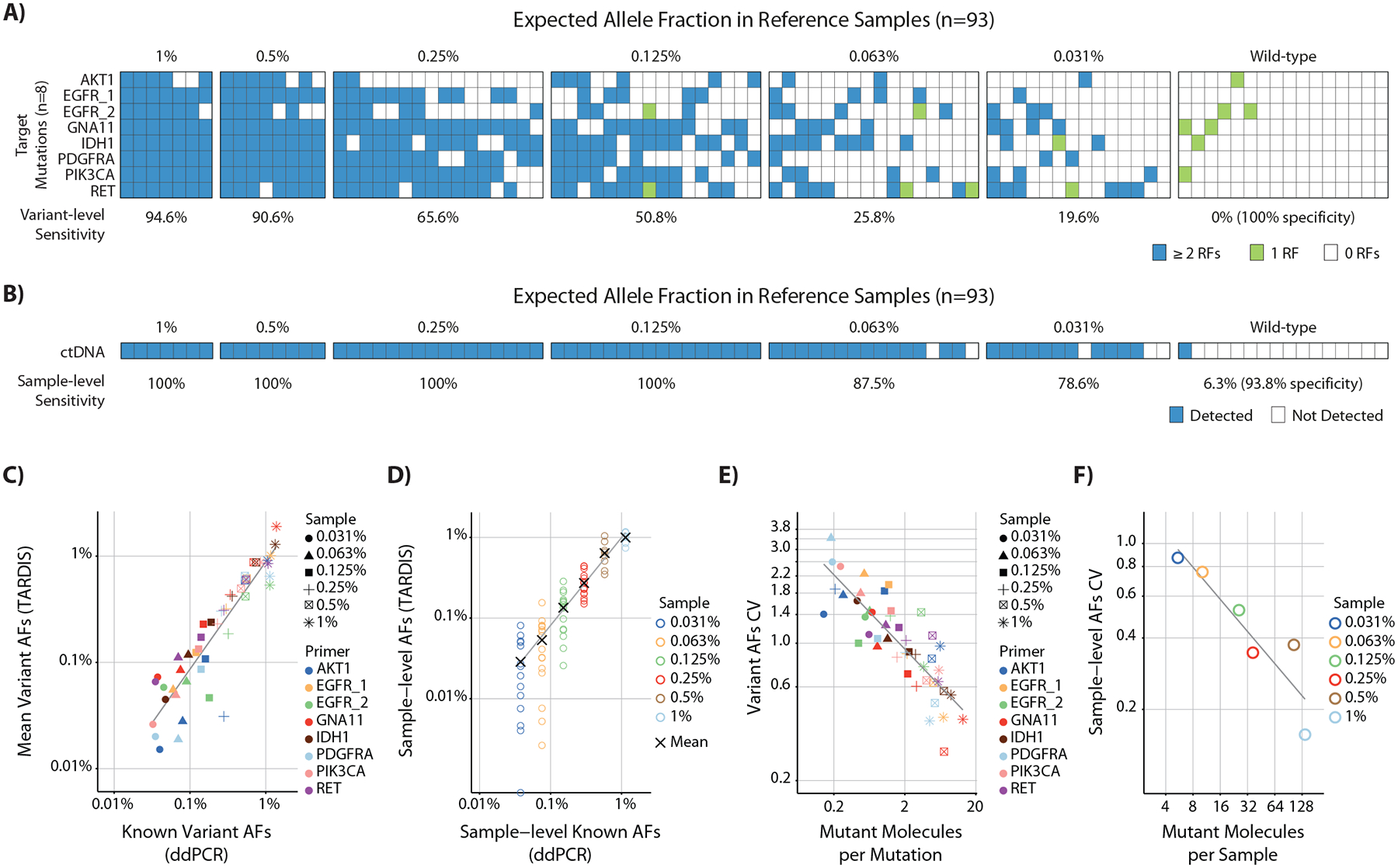
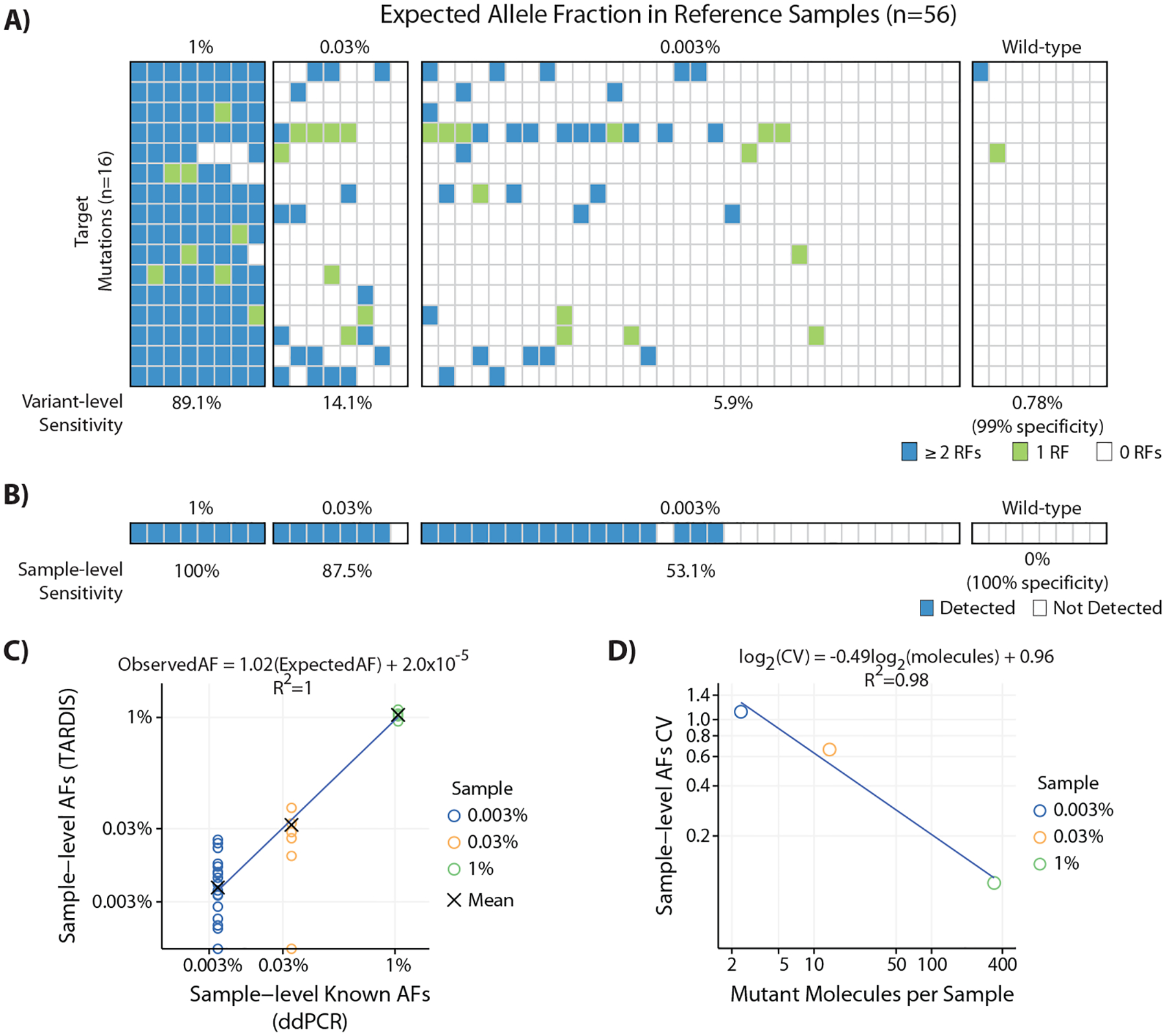
Longitudinal analysis of circulating tumor DNA (ctDNA) has shown promise for monitoring treatment response. However, most current methods lack adequate sensitivity for residual disease detection during or after completion of treatment in patients with nonmetastatic cancer. To address this gap and to improve sensitivity for minute quantities of residual tumor DNA in plasma, we have developed targeted digital sequencing (TARDIS) for multiplexed analysis of patient-specific cancer mutations. In reference samples, by simultaneously analyzing 8 to 16 known mutations, TARDIS achieved 91 and 53% sensitivity at mutant allele fractions (AFs) of 3 in 104 and 3 in 105, respectively, with 96% specificity, using input DNA equivalent to a single tube of blood. We successfully analyzed up to 115 mutations per patient in 80 plasma samples from 33 women with stage I to III breast cancer. Before treatment, TARDIS detected ctDNA in all patients with 0.11% median AF. After completion of neoadjuvant therapy, ctDNA concentrations were lower in patients who achieved pathological complete response (pathCR) compared to patients with residual disease (median AFs, 0.003 and 0.017%, respectively, P = 0.0057, AUC = 0.83). In addition, patients with pathCR showed a larger decrease in ctDNA concentrations during neoadjuvant therapy. These results demonstrate high accuracy for assessment of molecular response and residual disease during neoadjuvant therapy using ctDNA analysis. TARDIS has achieved up to 100-fold improvement beyond the current limit of ctDNA detection using clinically relevant blood volumes, demonstrating that personalized ctDNA tracking could enable individualized clinical management of patients with cancer treated with curative intent.
Copyright © 2019 The Authors, some rights reserved; exclusive licensee American Association for the Advancement of Science. No claim to original U.S. Government Works.
Conflict of interest statement
Figures



Comment in
-
Personalized MRD assays and therapy?Nat Rev Clin Oncol. 2019 Oct;16(10):593. doi: 10.1038/s41571-019-0269-2. Nat Rev Clin Oncol. 2019. PMID: 31435000 No abstract available.
-
Fastidious Detection of Circulating Tumor DNA Mutations in Residual Breast Cancer Disease for Ultimate Analytical Sensitivity and Specificity.Clin Chem. 2020 Jul 1;66(7):866-867. doi: 10.1093/clinchem/hvaa068. Clin Chem. 2020. PMID: 32215639 No abstract available.
References
-
- Katz SJ, Jagsi R, Morrow M, Reducing Overtreatment of Cancer With Precision Medicine: Just What the Doctor Ordered. JAMA 319, 1091–1092 (2018). - PubMed
-
- Cortazar P, Zhang L, Untch M, Mehta K, Costantino J, Wolmark N, Bonnefoi H, Cameron D, Gianni L, Valagussa P, Meta-analysis results from the collaborative trials in neoadjuvant breast cancer (CTNeoBC). Cancer Res 72, S1–S11 (2012).
-
- Symmans WF, Wei C, Gould R, Yu X, Zhang Y, Liu M, Walls A, Bousamra A, Ramineni M, Sinn B, Hunt K, Buchholz TA, Valero V, Buzdar AU, Yang W, Brewster AM, Moulder S, Pusztai L, Hatzis C, Hortobagyi GN, Long-Term Prognostic Risk After Neoadjuvant Chemotherapy Associated With Residual Cancer Burden and Breast Cancer Subtype. J Clin Oncol 35, 1049–1060 (2017). - PMC - PubMed
-
- Chagpar AB, Middleton LP, Sahin AA, Dempsey P, Buzdar AU, Mirza AN, Ames FC, Babiera GV, Feig BW, Hunt KK, Kuerer HM, Meric-Bernstam F, Ross MI, Singletary SE, Accuracy of physical examination, ultrasonography, and mammography in predicting residual pathologic tumor size in patients treated with neoadjuvant chemotherapy. Annals of surgery 243, 257–264 (2006). - PMC - PubMed
-
- Yuan Y, Chen XS, Liu SY, Shen KW, Accuracy of MRI in prediction of pathologic complete remission in breast cancer after preoperative therapy: a meta-analysis. AJR. American journal of roentgenology 195, 260–268 (2010). - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
