

Complications of Insufficient Dura and Blood Loss During Surgical Intervention in Shprintzen-Goldberg Syndrome: A Case Report
- PMID: 31391415
- PMCID: PMC6698069
- DOI: 10.12659/AJCR.914924
Complications of Insufficient Dura and Blood Loss During Surgical Intervention in Shprintzen-Goldberg Syndrome: A Case Report
Abstract
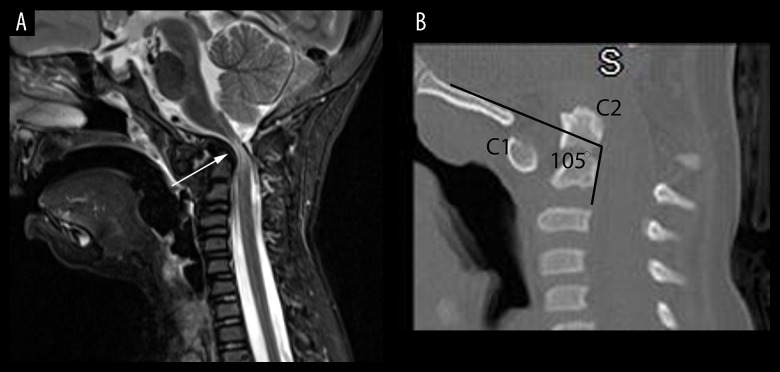
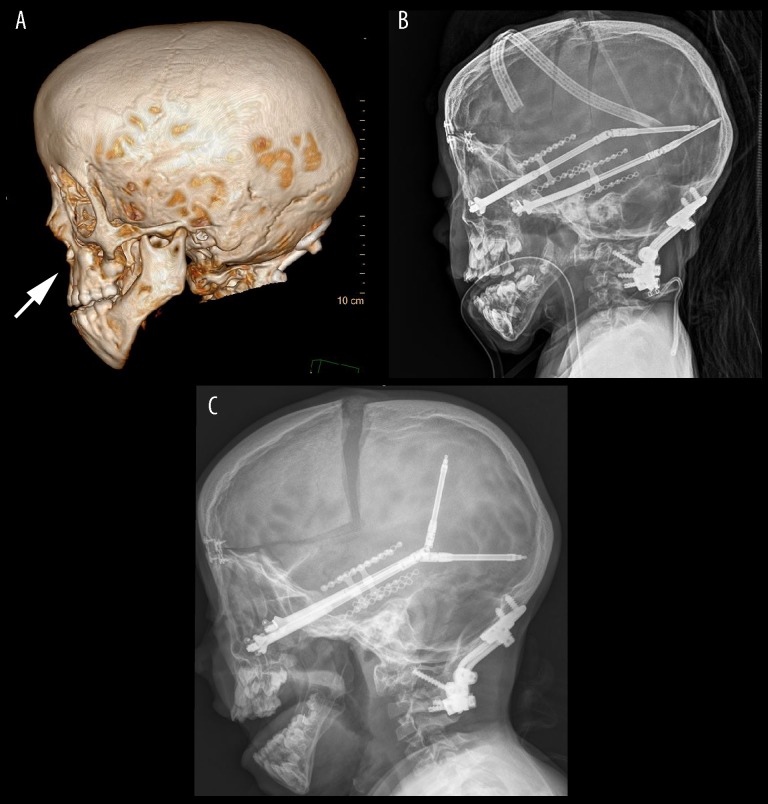
BACKGROUND Shprintzen-Goldberg syndrome (SGS) is an extremely rare collagenopathy, most often caused by autosomal-dominant mutations in the SKI proto-oncogene, which is a component of the transforming growth factor beta (TGF-ß) signaling pathway. Approximately 50-60 cases of SGS have been recorded in the literature worldwide since its discovery in 1982. This collagen disorder affects bone and vascular development throughout the body, resulting in craniosynostosis, scoliosis, chest deformities, and aortic root dilation. Patients may have problems in the central nervous system, including Chiari 1 malformation, hydrocephalus, and dilation of the lateral ventricles. Unfortunately, the symptoms of SGS closely parallel those of related collagenopathies involving mutations in the TGF-ß signaling pathway, which makes accurate diagnosis difficult without genetic testing, especially in cases with complex presentation. CASE REPORT In this report we present the unique and complex disease manifestations in a 9-year-old girl with SGS. The patient had severe cervical spinal instability that resolved after surgical occipital-C4 fusion with an autograft from the rib. Midface distraction surgery was used to treat the patient's craniosynostosis and related facial deformities. This surgery was complicated by loss of 750 mL of blood due to insufficient dura and prominent vasculature. CONCLUSIONS Connective tissue symptoms associated with SGS can involve dural and vascular problems, as seen in this case report. Thus, the risk of extreme blood loss should be anticipated any time midface distraction surgery is performed on an SGS patient. Continued research is needed to define how this case relates to the SGS patient population.
Conflict of interest statement
None.
Figures
References
-
- Kinaci A, Algra A, Heuts S, et al. Effectiveness of dural sealants in prevention of CSF leakage after craniotomy: A systematic review. World Neurosurg. 2018;118:368–76. - PubMed
-
- Laure B, Moret A, Joly A, et al. Orbitofrontal monobloc advancement for Crouzon syndrome. J Cranio Maxill Surg. 2014;42(6):335–38. - PubMed
Publication types
MeSH terms
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
