

Sarcopenia in cirrhosis: from pathogenesis to interventions
- PMID: 31392488
- PMCID: PMC6759678
- DOI: 10.1007/s00535-019-01605-6
Sarcopenia in cirrhosis: from pathogenesis to interventions
Abstract
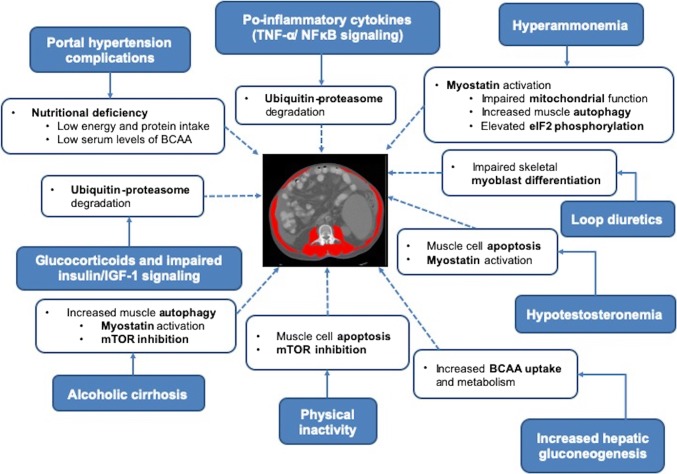
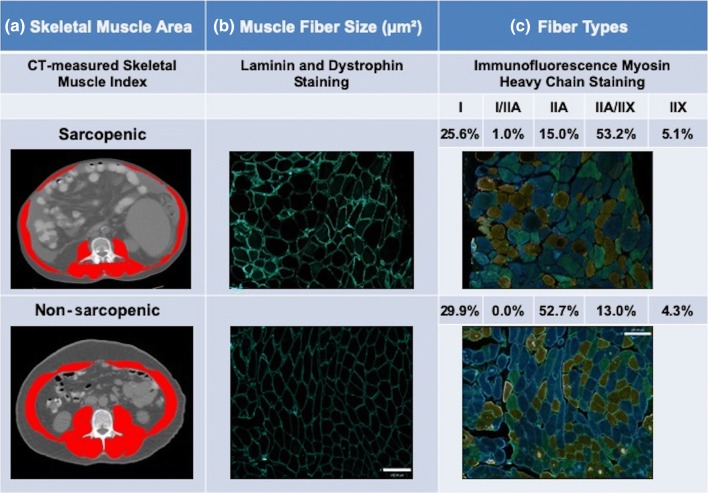
Sarcopenia (severe muscle depletion) is a prevalent muscle abnormality in patients with cirrhosis that confers poor prognosis both pre- and post-liver transplantation. The pathogenesis of sarcopenia is multifactorial and results from an imbalance between protein synthesis and breakdown. Nutritional, metabolic, and biochemical abnormalities seen in chronic liver disease alter whole body protein homeostasis. Hyperammonemia, increased autophagy, proteasomal activity, lower protein synthesis, and impaired mitochondrial function play an important role in muscle depletion in cirrhosis. Factors including cellular energy status, availability of metabolic substrates (e.g., branched-chain amino acids), alterations in the endocrine system (insulin resistance, circulating levels of insulin, insulin-like growth factor-1, corticosteroids, and testosterone), cytokines, myostatin, and exercise are involved in regulating muscle mass. A favored atrophy of type II fast-twitch glycolytic fibers seems to occur in patients with cirrhosis and sarcopenia. Identification of muscle biological abnormalities and underlying mechanisms is required to plan clinical trials to reverse sarcopenia through modulation of specific mechanisms. Accordingly, a combination of nutritional, physical, and pharmacological interventions might be necessary to reverse sarcopenia in cirrhosis. Moderate exercise should be combined with appropriate energy and protein intake, in accordance with clinical guidelines. Interventions with branched chain amino acids, testosterone, carnitine, or ammonia-lowering therapies should be considered individually. Various factors such as dose, type, duration of supplementations, etiology of cirrhosis, amount of dietary protein intake, and compliance with supplementation and exercise should be the focus of future large randomized controlled trials investigating both prevention and treatment of sarcopenia in this patient population.
Keywords: Interventions; Mechanisms; Muscle loss; Pathways.
Conflict of interest statement
All authors declare that they have no conflict of interest.
Figures
References
-
- Shen W, Punyanitya M, Wang Z, et al. Total body skeletal muscle and adipose tissue volumes: estimation from a single abdominal cross-sectional image. J Appl Physiol. 2004;97:2333–2338. - PubMed
-
- Mitsiopoulos N, Baumgartner RN, Heymsfield SB, et al. Cadaver validation of skeletal muscle measurement by magnetic resonance imaging and computerized tomography. J Appl Physiol. 1998;85:115–122. - PubMed
-
- van Vugt JLA, Coebergh van den Braak RRJ, Schippers HJW, et al. Contrast-enhancement influences skeletal muscle density, but not skeletal muscle mass, measurements on computed tomography. Clin Nutr. 2018;37:1707–1714. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
