

Evaluation and Predictors of Fluid Resuscitation in Patients With Severe Sepsis and Septic Shock
- PMID: 31393324
- PMCID: PMC8096207
- DOI: 10.1097/CCM.0000000000003960
Evaluation and Predictors of Fluid Resuscitation in Patients With Severe Sepsis and Septic Shock
Abstract
Objectives: Rapid fluid resuscitation has become standard in sepsis care, despite "low-quality" evidence and absence of guidelines for populations "at risk" for volume overload. Our objectives include as follows: 1) identify predictors of reaching a 30 mL/kg crystalloid bolus within 3 hours of sepsis onset (30by3); 2) assess the impact of 30by3 and fluid dosing on clinical outcomes; 3) examine differences in perceived "at-risk" volume-sensitive populations, including end-stage renal disease, heart failure, obesity, advanced age, or with documentation of volume "overload" by bedside examination.
Design: Retrospective cohort study. All outcome analyses controlled for sex, end-stage renal disease, heart failure, sepsis severity (severe sepsis vs septic shock), obesity, Mortality in Emergency Department Sepsis score, and time to antibiotics.
Setting: Urban, tertiary care center between January 1, 2014, and May 31, 2017.
Patients: Emergency Department treated adults (age ≥18 yr; n = 1,032) with severe sepsis or septic shock.
Interventions: Administration of IV fluids by bolus.
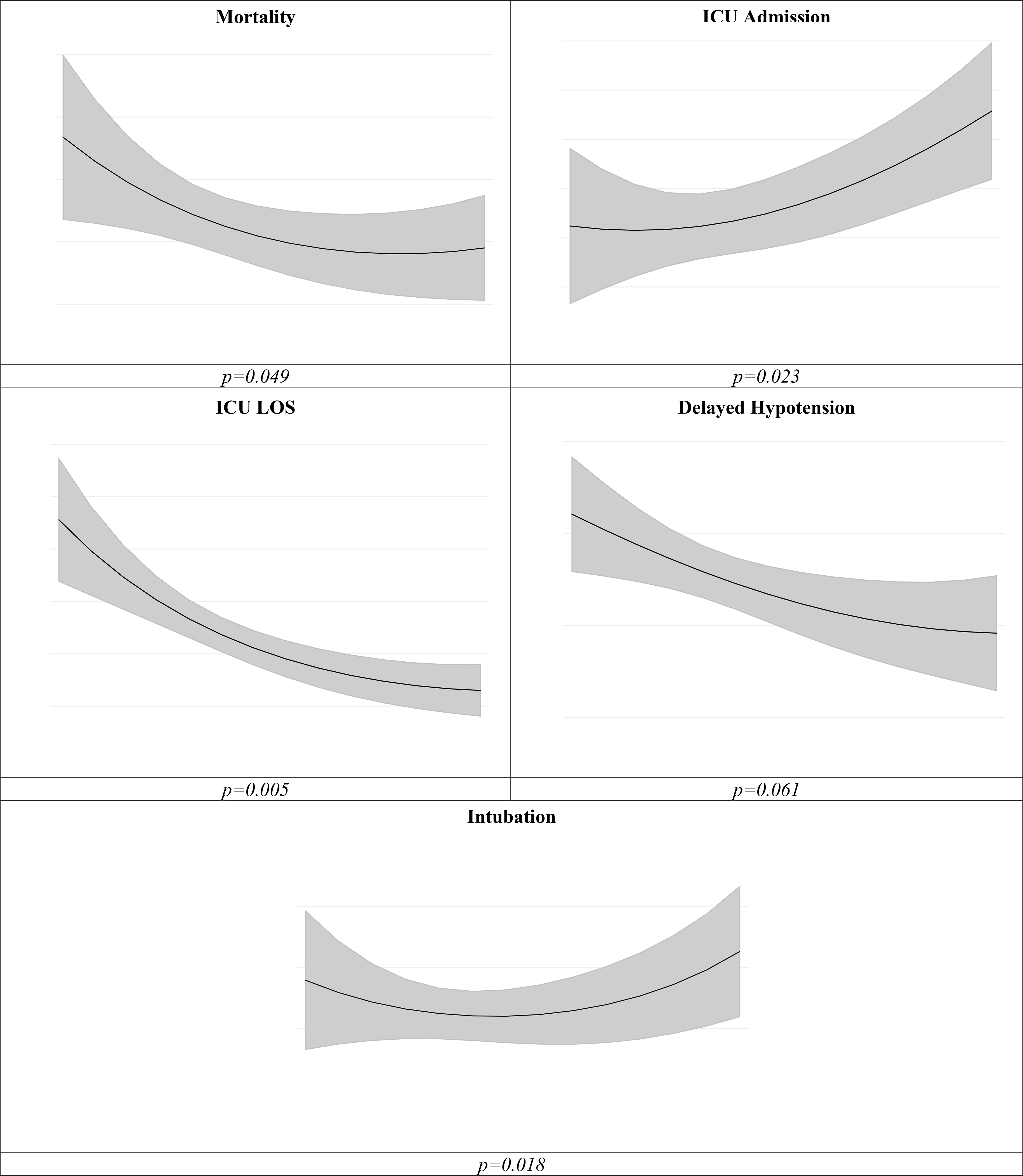
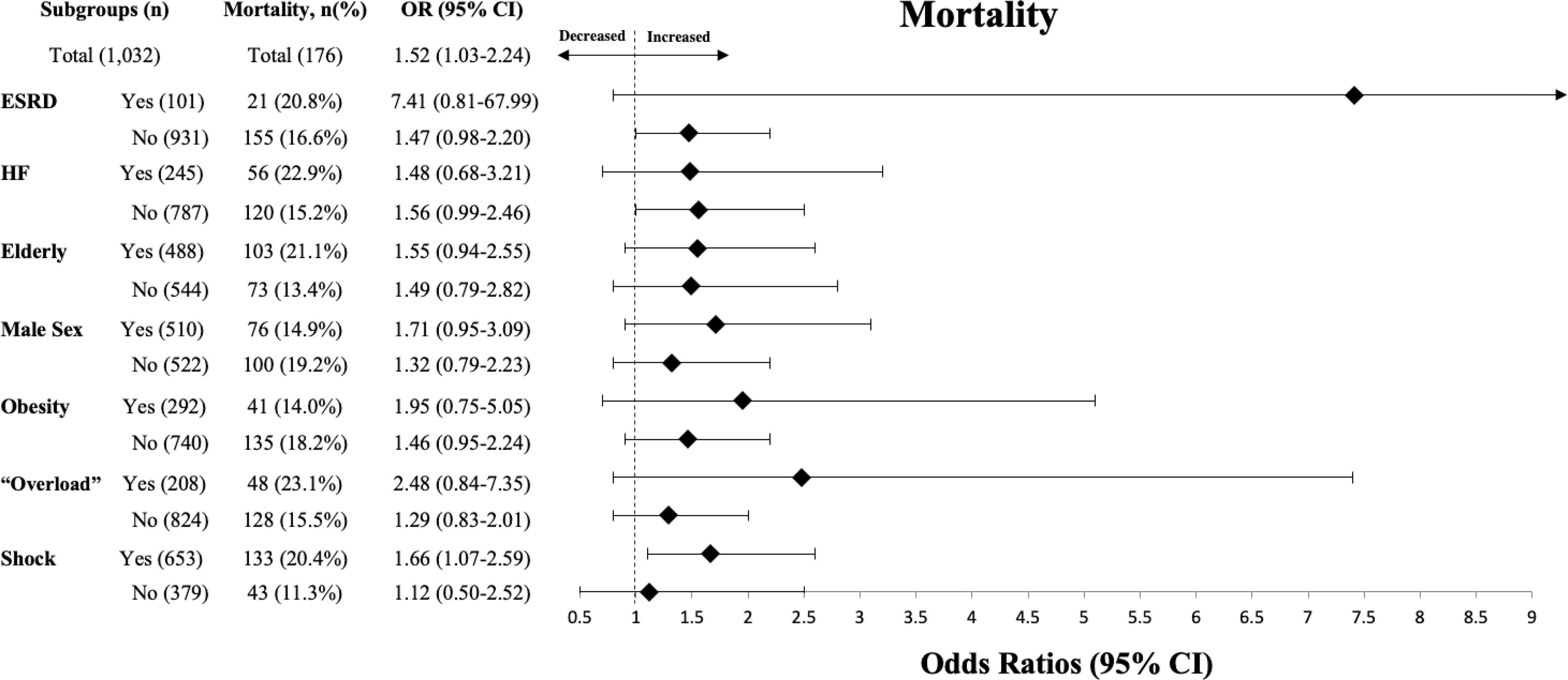
Measurements and main results: In total, 509 patients received 30by3 (49.3%). Overall mortality was 17.1% (n = 176), with 20.4% mortality in the shock group. Patients who were elderly (odds ratio, 0.62; 95% CI, 0.46-0.83), male (odds ratio, 0.66; CI, 0.49-0.87), obese (odds ratio, 0.18; CI, 0.13-0.25), or with end-stage renal disease (odds ratio, 0.23; CI, 0.13-0.40), heart failure (odds ratio, 0.42; CI, 0.29-0.60), or documented volume "overload" (odds ratio, 0.30; CI, 0.20-0.45) were less likely to achieve 30by3. Failure to meet 30by3 had increased odds of mortality (odds ratio, 1.52; CI, 1.03-2.24), delayed hypotension (odds ratio, 1.42; CI, 1.02-1.99), and increased ICU stay (~2 d) (β = 2.0; CI, 0.5-3.6), without differential effects for "at-risk" groups. Higher fluid volumes administered by 3 hours correlated with decreased mortality, with a plateau effect between 35 and 45 mL/kg (p < 0.05).
Conclusions: Failure to reach 30by3 was associated with increased odds of in-hospital mortality, irrespective of comorbidities. Predictors of inadequate resuscitation can be identified, potentially leading to interventions to improve survival. These findings are retrospective and require future validation.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
Comment in
-
Getting to the Heart of the Matter: What We Know About Fluid Resuscitation in Septic Heart Failure Patients.Crit Care Med. 2020 Mar;48(3):e259-e260. doi: 10.1097/CCM.0000000000004126. Crit Care Med. 2020. PMID: 32058403 Free PMC article. No abstract available.
-
The authors reply.Crit Care Med. 2020 Mar;48(3):e260-e261. doi: 10.1097/CCM.0000000000004184. Crit Care Med. 2020. PMID: 32058404 No abstract available.
References
-
- Rivers E, Nguyen B, Havstad S, et al.: Early Goal-Directed Therapy in the Treatment of Severe Sepsis and Septic Shock. N Engl J Med 2001; 345:1368–1377 - PubMed
-
- Peake SL, Delaney A, Bailey M, et al.: Goal-directed resuscitation for patients with early septic shock. N Engl J Med 2014; 371:1496–1506 - PubMed
-
- Mouncey PR, Osborn TM, Power GS, et al.: Trial of Early, Goal-Directed Resuscitation for Septic Shock. N Engl J Med 2015; 372:1301–1311 - PubMed
-
- Levy MM, Rhodes A, Phillips GS, et al.: Surviving Sepsis Campaign: association between performance metrics and outcomes in a 7.5-year study. Crit Care Med 2015; 43:3–12 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
