

Serum magnesium levels during magnesium sulfate infusion at 1 gram/hour versus 2 grams/hour as a maintenance dose to prevent eclampsia in women with severe preeclampsia: A randomized clinical trial
- PMID: 31393402
- PMCID: PMC6709127
- DOI: 10.1097/MD.0000000000016779
Serum magnesium levels during magnesium sulfate infusion at 1 gram/hour versus 2 grams/hour as a maintenance dose to prevent eclampsia in women with severe preeclampsia: A randomized clinical trial
Abstract
Background: Magnesium sulfate is the ideal drug for the prevention and treatment of eclampsia. Nevertheless, the best regimen for protection against eclampsia with minimal side effects remains to be established. This study aimed to compare serum magnesium levels during intravenous infusion of magnesium sulfate at 1 gram/hour versus 2 grams/hour as a maintenance dose to prevent eclampsia in pregnant and postpartum women with severe preeclampsia.
Methods: A randomized, triple-blind clinical trial was conducted, comparing serum magnesium levels during the intravenous infusion of magnesium sulfate at 1 gram/hour versus 2 grams/hour as a maintenance dose for the prevention of eclampsia in 62 pregnant and postpartum women with severe preeclampsia, 31 in each group. An intravenous loading dose of 6 grams of magnesium sulfate was administered over 30 minutes in both groups. The patients were then randomized to receive a maintenance dose of either 1 or 2 grams/hour for 24 hours. Primary outcomes consisted of serum magnesium levels at the following time points: baseline, 30 minutes, every 2 hours until the end of the first 6 hours, and every 6 hours thereafter until the termination of magnesium sulfate infusion. Side effects, maternal complications, and neonatal outcomes were the secondary outcomes.
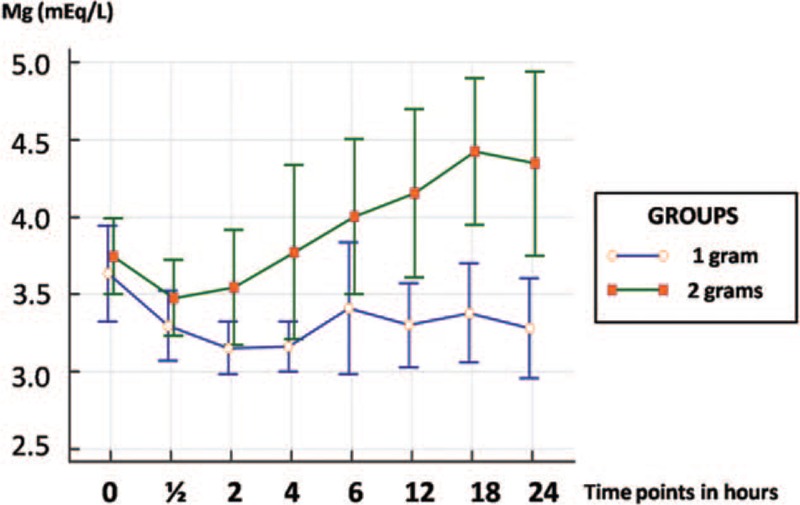
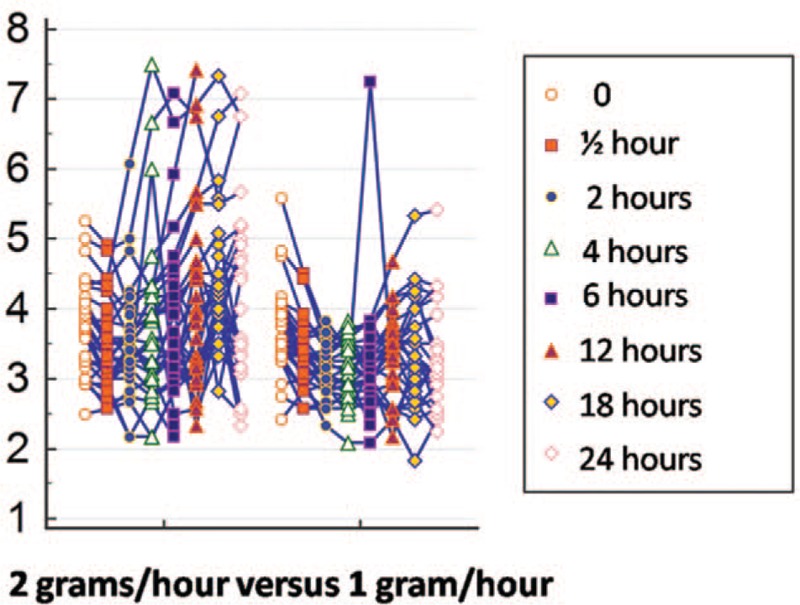
Results: Serum magnesium levels were higher in the 2-gram/hour group, with a statistically significant difference from 2 hours after the beginning of the magnesium sulfate infusion (P <.05). Oliguria was the most common complication recorded in both groups, with no significant difference between the 2 regimens (RR 0.88; 95% CI: 0.49-1.56; P = .65). No cases of eclampsia occurred. Side effects were more common in the 2-gram/hour group (RR 1.89; 95% CI: 1.04-3.41; P = .02); however, all were mild. There were no differences between the 2 groups regarding neonatal outcomes, except for admission to neonatal intensive care, which was more frequent in the 1-gram/hour group (25% vs 6.3%; P = .04).
Conclusion: Magnesium sulfate therapy at the maintenance dose of 1 gram/hour was just as effective as the 2-gram maintenance dose, with fewer side effects.
Conflict of interest statement
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
Figures

References
-
- Ghulmiyyah L, Sibai B. Maternal mortality from preeclampsia/eclampsia. Semin Perinatol 2012;36:56–9. - PubMed
-
- Steegers EA, Von Dadelszen P, Duvekot JJ, et al. Pre-eclampsia. Lancet 2010;376:631–44. - PubMed
-
- Duley L. Maternal mortality associated with hypertensive disorders of pregnancy in Africa, Asia, Latin America and the Caribbean. Br J Obstet Gynaecol 1992;99:547–53. - PubMed
-
- Duley L. The global impact of pre-eclampsia and eclampsia. Semin Perinatol 2009;33:130–7. - PubMed
-
- Vigil-De Gracia P. Maternal deaths due to eclampsia and HELLP syndrome. Int J Gynaecol Obstet 2009;104:90–4. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
