

A placebo-controlled randomized study with testosterone in Klinefelter syndrome: beneficial effects on body composition
- PMID: 31394497
- PMCID: PMC6733367
- DOI: 10.1530/EC-19-0323
A placebo-controlled randomized study with testosterone in Klinefelter syndrome: beneficial effects on body composition
Abstract
Context and objective: Males with Klinefelter syndrome (KS) are typically hypogonadal with a high incidence of metabolic disease, increased body fat and mortality. Testosterone treatment of hypogonadal patients decrease fat mass, increase lean body mass and improve insulin sensitivity, but whether this extends to patients with KS is presently unknown.
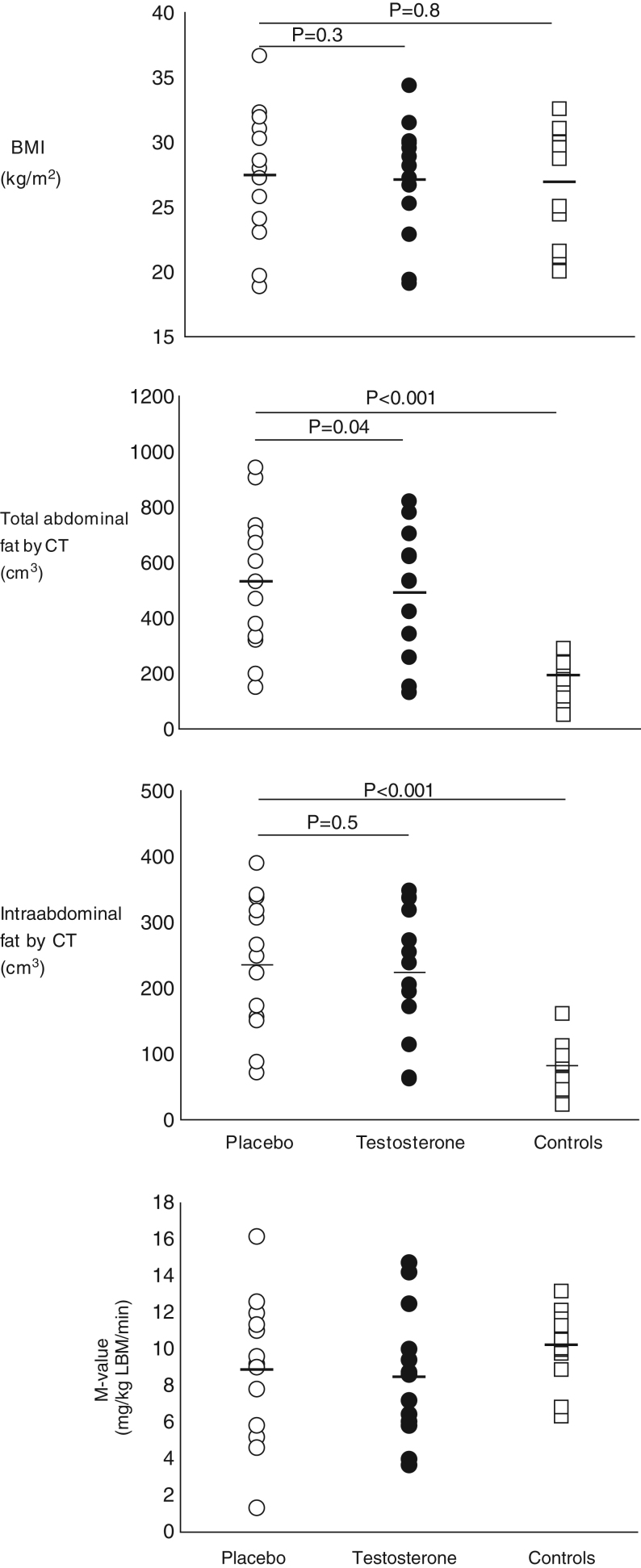
Research design and methods: In a randomized, double-blind, placebo-controlled, BMI-matched cross-over study, 13 males with KS (age: 34.8 years; BMI: 26.7 kg/m2) received testosterone (Andriol®) 160 mg per day (testosterone) or placebo treatment for 6 months. Thirteen age- and BMI-matched healthy controls were recruited. DEXA scan, abdominal computed tomography (CT) scan and a hyperinsulinemic-euglycemic clamp, muscle strength and maximal oxygen uptake measurement were performed.
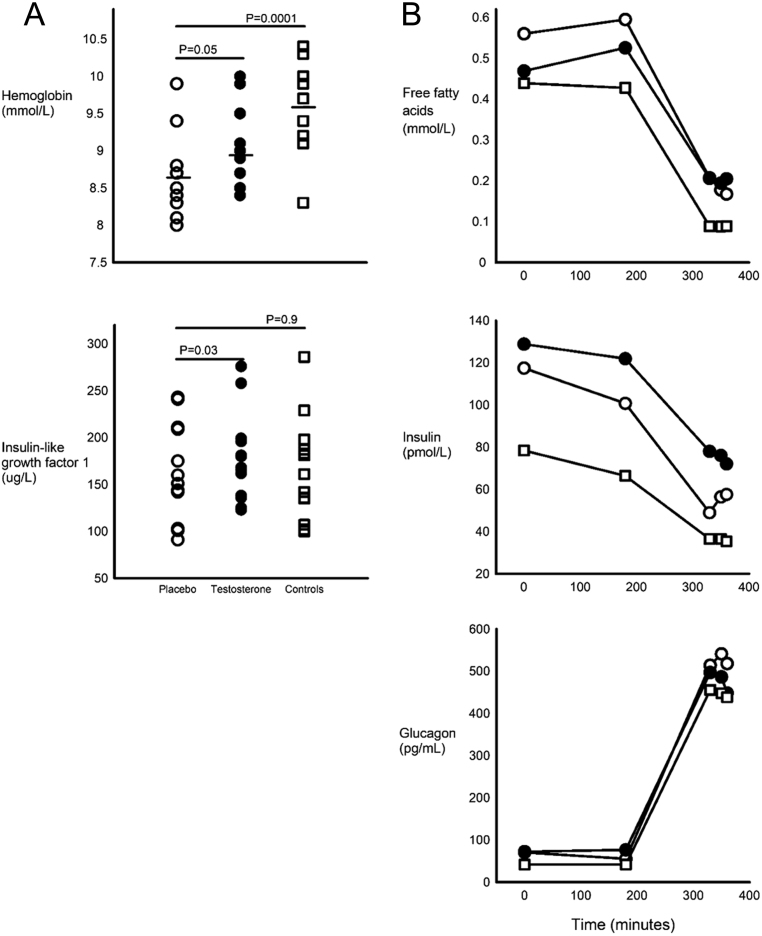
Results: Total lean body mass and body fat mass were comparable between testosterone-naïve KS and controls using DEXA, whereas visceral fat mass, total abdominal and intra-abdominal fat by CT was increased (P < 0.05). Testosterone decreased total body fat (P = 0.01) and abdominal fat by CT (P = 0.04). Glucose disposal was similar between testosterone-naïve KS and controls (P = 0.3) and unchanged during testosterone (P = 0.8). Free fatty acid suppression during the clamp was impaired in KS and maximal oxygen uptake was markedly lower in KS, but both were unaffected by treatment. Testosterone increased hemoglobin and IGF-I.
Conclusion: Testosterone treatment in adult males with KS for 6 months leads to favorable changes in body composition with reductions in fat mass, including abdominal fat mass, but does not change measures of glucose homeostasis.
Keywords: Klinefelter syndrome; body composition; insulin sensitivity; rare diseases/syndromes; testosterone.
Figures

References
-
- Bojesen A, Kristensen K, Birkebaek NH, Fedder J, Mosekilde L, Bennett P, Laurberg P, Frystyk J, Flyvbjerg A, Christiansen JS, et al. The metabolic syndrome is frequent in Klinefelter’s syndrome and is associated with abdominal obesity and hypogonadism. Diabetes Care 2006. 1591–1598. ( 10.2337/dc06-0145) - DOI - PubMed
LinkOut - more resources
Full Text Sources
