

Diet in Irritable Bowel Syndrome (IBS): Interaction with Gut Microbiota and Gut Hormones
- PMID: 31394793
- PMCID: PMC6723613
- DOI: 10.3390/nu11081824
Diet in Irritable Bowel Syndrome (IBS): Interaction with Gut Microbiota and Gut Hormones
Abstract
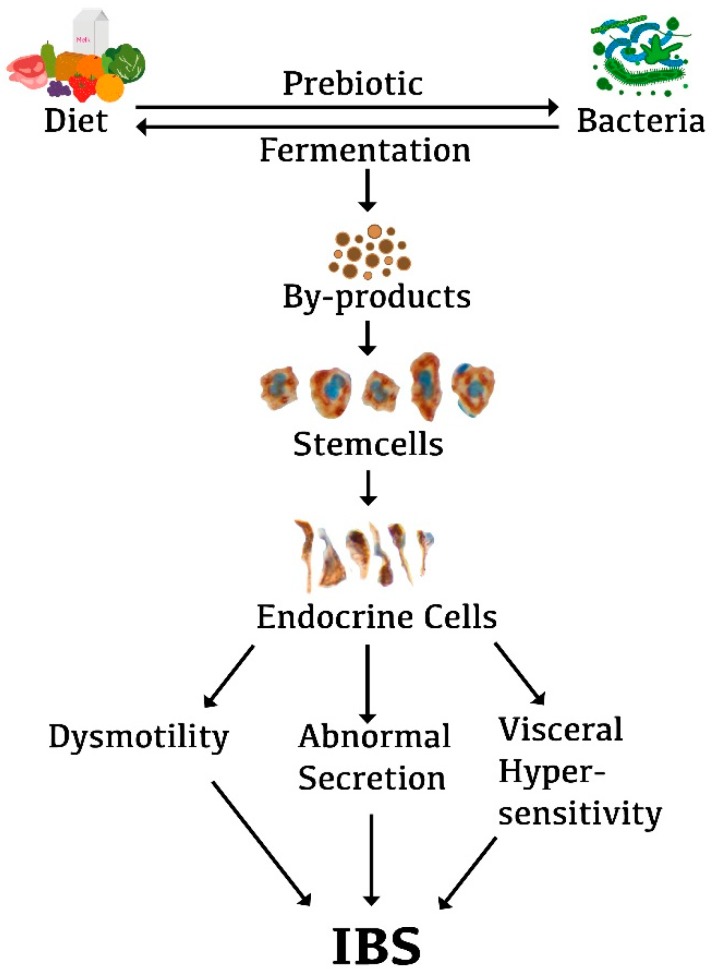
Diet plays an important role not only in the pathophysiology of irritable bowel syndrome (IBS), but also as a tool that improves symptoms and quality of life. The effects of diet seem to be a result of an interaction with the gut bacteria and the gut endocrine cells. The density of gut endocrine cells is low in IBS patients, and it is believed that this abnormality is the direct cause of the symptoms seen in IBS patients. The low density of gut endocrine cells is probably caused by a low number of stem cells and low differentiation progeny toward endocrine cells. A low fermentable oligo-, di-, monosaccharide, and polyol (FODMAP) diet and fecal microbiota transplantation (FMT) restore the gut endocrine cells to the level of healthy subjects. It has been suggested that our diet acts as a prebiotic that favors the growth of a certain types of bacteria. Diet also acts as a substrate for gut bacteria fermentation, which results in several by-products. These by-products might act on the stem cells in such a way that the gut stem cells decrease, and consequently, endocrine cell numbers decrease. Changing to a low-FODMAP diet or changing the gut bacteria through FMT improves IBS symptoms and restores the density of endocrine cells.
Keywords: IBS; diet; fecal microbiota transplantation; gut endocrine cells; gut microbiota.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
