

Immunogenicity of pembrolizumab in patients with advanced tumors
- PMID: 31395089
- PMCID: PMC6686242
- DOI: 10.1186/s40425-019-0663-4
Immunogenicity of pembrolizumab in patients with advanced tumors
Abstract
Background: Pembrolizumab is a potent, humanized, monoclonal anti-programmed death 1 antibody that has demonstrated effective antitumor activity and acceptable safety in multiple tumor types. Therapeutic biologics can result in the development of antidrug antibodies (ADAs), which may alter drug clearance and neutralize target binding, potentially reducing drug efficacy; such immunogenicity may also result in infusion reactions, anaphylaxis, and immune complex disorders. Pembrolizumab immunogenicity and its impact on exposure, safety, and efficacy was assessed in this study.
Patients and methods: Pembrolizumab immunogenicity was assessed in 3655 patients with advanced or metastatic cancer treated in 12 clinical studies. Patients with melanoma, non-small cell lung cancer, head and neck squamous cell carcinoma, colorectal cancer, urothelial cancer, and Hodgkin lymphoma were treated with pembrolizumab at 2 mg/kg every 3 weeks, 10 mg/kg every 2 weeks, 10 mg/kg every 3 weeks, or 200 mg every 3 weeks. An additional study involving 496 patients with stage III melanoma treated with 200 mg adjuvant pembrolizumab every 3 weeks after complete resection was analyzed separately.
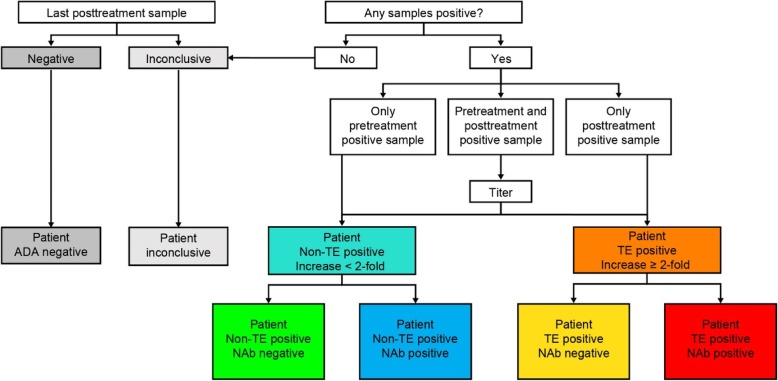
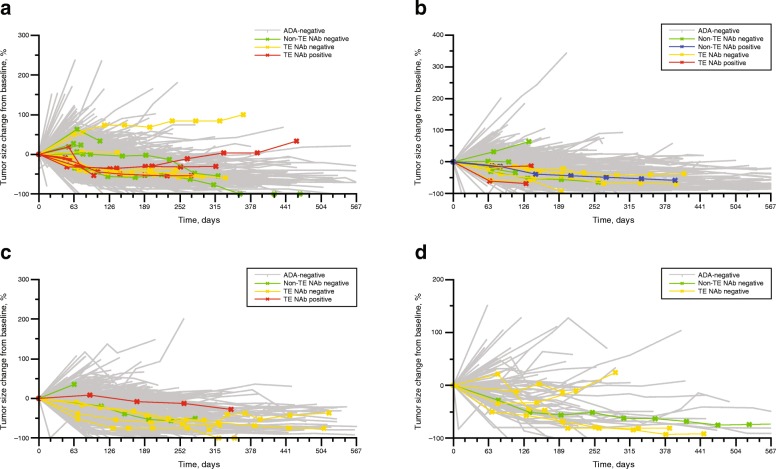
Results: Of 3655 patients, 2000 were evaluable for immunogenicity analysis, 36 (1.8%) were treatment-emergent (TE) ADA-positive; 9 (0.5%) of these TE-positive patients had antibodies with neutralizing capacity. The presence of pembrolizumab-specific ADAs did not impact pembrolizumab exposure, nor did pembrolizumab immunogenicity affect the incidence of drug-related adverse events (AEs) or infusion-related reactions. There was no clear relationship between the presence of pembrolizumab-specific ADAs and changes in tumor size across treatment regimens. Of the 496 patients treated with pembrolizumab as adjuvant therapy, 495 were evaluable, 17 (3.4%) were TE ADA-positive; none had neutralizing antibodies.
Conclusions: The incidence of TE (neutralizing positive) ADAs against pembrolizumab was low in patients with advanced tumors. Furthermore, immunogenicity did not appear to have any clinically relevant effects on the exposure, safety, or efficacy of pembrolizumab.
Trial registration: ClinicalTrials.gov, NCT01295827 (February 15, 2011), NCT01704287 (October 11, 2012), NCT01866319 (May 31, 2013), NCT01905657 (July 23, 2013), NCT02142738 (May 20, 2014), NCT01848834 (May 8, 2013), NCT02255097 (October 2, 2014), NCT02460198 (June 2, 2015), NCT01953692 (October 1, 2013), NCT02453594 (May 25, 2015), NCT02256436 (October 3, 2014), NCT02335424 (January 9, 2015), NCT02362594 (February 13, 2015).
Keywords: Advanced tumors; Efficacy; Immunogenicity; Pembrolizumab; Safety; Treatment-emergent ADA.
Conflict of interest statement
LL, DCT, AC, ML, M. Li, SHR, AGK, DDA, KM, LJ, and TF are current or former employees of Merck Sharp & Dohme Corp., a subsidiary of Merck & Co., Inc., Kenilworth, NJ, USA. JAS and ESS are employees of Merck Sharp & Dohme Corp., a subsidiary of Merck & Co., Inc., Kenilworth, NJ, USA, and hold stock in the company. MJHvV and HJMMdG have nothing to disclose. DCT was an employee of Merck Sharp & Dohme Corp., a subsidiary of Merck & Co., Inc., Kenilworth, NJ at the time of the analysis and is currently employed by GlaxoSmithKline, and M. Li was an employee of Merck Sharp & Dohme Corp., a subsidiary of Merck & Co., Inc., Kenilworth, NJ at the time of the analysis and is currently employed by Sanofi.
Figures
References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials