

Infant mortality: the contribution of genetic disorders
- PMID: 31395954
- PMCID: PMC6879816
- DOI: 10.1038/s41372-019-0451-5
Infant mortality: the contribution of genetic disorders
Abstract
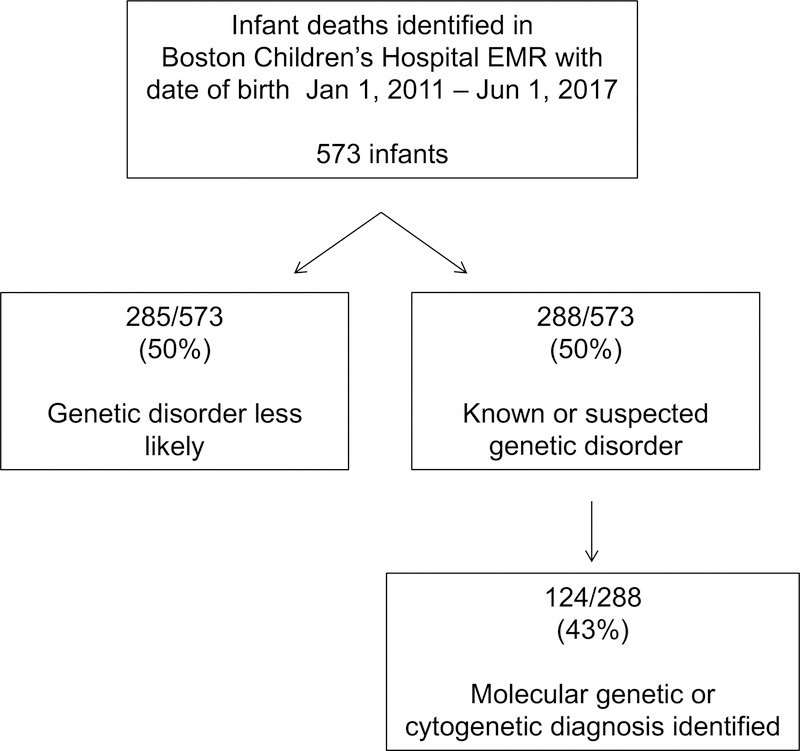
Objective: To determine the proportion of infant deaths occurring in the setting of a confirmed genetic disorder.
Study design: A retrospective analysis of the electronic medical records of infants born from 1 January, 2011 to 1 June, 2017, who died prior to 1 year of age.
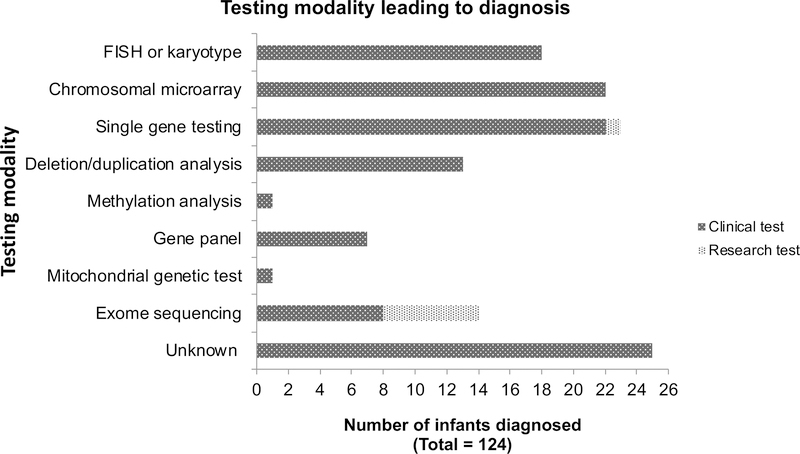
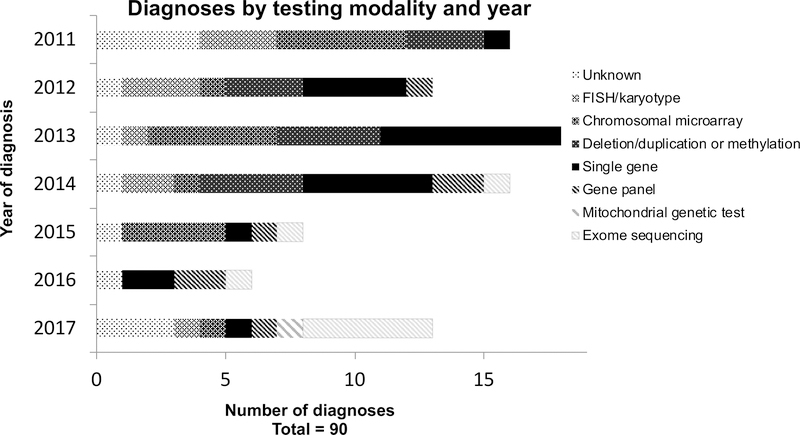
Results: Five hundred and seventy three deceased infants were identified. One hundred and seventeen were confirmed to have a molecular or cytogenetic diagnosis in a clinical diagnostic laboratory and an additional seven were diagnosed by research testing for a total of 124/573 (22%) diagnosed infants. A total of 67/124 (54%) had chromosomal disorders and 58/124 (47%) had single gene disorders (one infant had both). The proportion of diagnoses made by sequencing technologies, such as exome sequencing, increased over the years.
Conclusions: The prevalence of confirmed genetic disorders within our cohort of infant deaths is higher than that previously reported. Increased efforts are needed to further understand the mortality burden of genetic disorders in infancy.
Conflict of interest statement
Potential Conflicts of Interest:
The authors have no conflicts of interest relevant to this article to disclose (Dr. Mullen is currently an employee of Quest Diagnostics who performed the work pertaining to this article while at the Broad Institute of MIT and Harvard).
Figures
References
-
- Simpson CD, Ye XY, Hellmann J, Tomlinson C. Trends in cause-specific mortality at a Canadian outborn NICU. Pediatrics 2010, 126(6): 1538. - PubMed
-
- Jacob J, Kamitsuka M, Clark RH, Kelleher AS, Spitzer AR. Etiologies of NICU deaths. Pediatrics 2015, 135(1): e59–65. - PubMed
-
- Meng M, Zhang YP. Impact of inborn errors of metabolism on admission in a neonatal intensive care unit: a 4-year report. J Pediatr Endocrinol Metab 2013, 26(7–8): 689–693. - PubMed
-
- Hudome SM, Kirby RS, Senner JW, Cunniff C. Contribution of genetic disorders to neonatal mortality in a regional intensive care setting. Am J Perinatol 1994, 11(2): 100–103. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
