

Evans Syndrome in Childhood: Long Term Follow-Up and the Evolution in Primary Immunodeficiency or Rheumatological Disease
- PMID: 31396497
- PMCID: PMC6664023
- DOI: 10.3389/fped.2019.00304
Evans Syndrome in Childhood: Long Term Follow-Up and the Evolution in Primary Immunodeficiency or Rheumatological Disease
Abstract
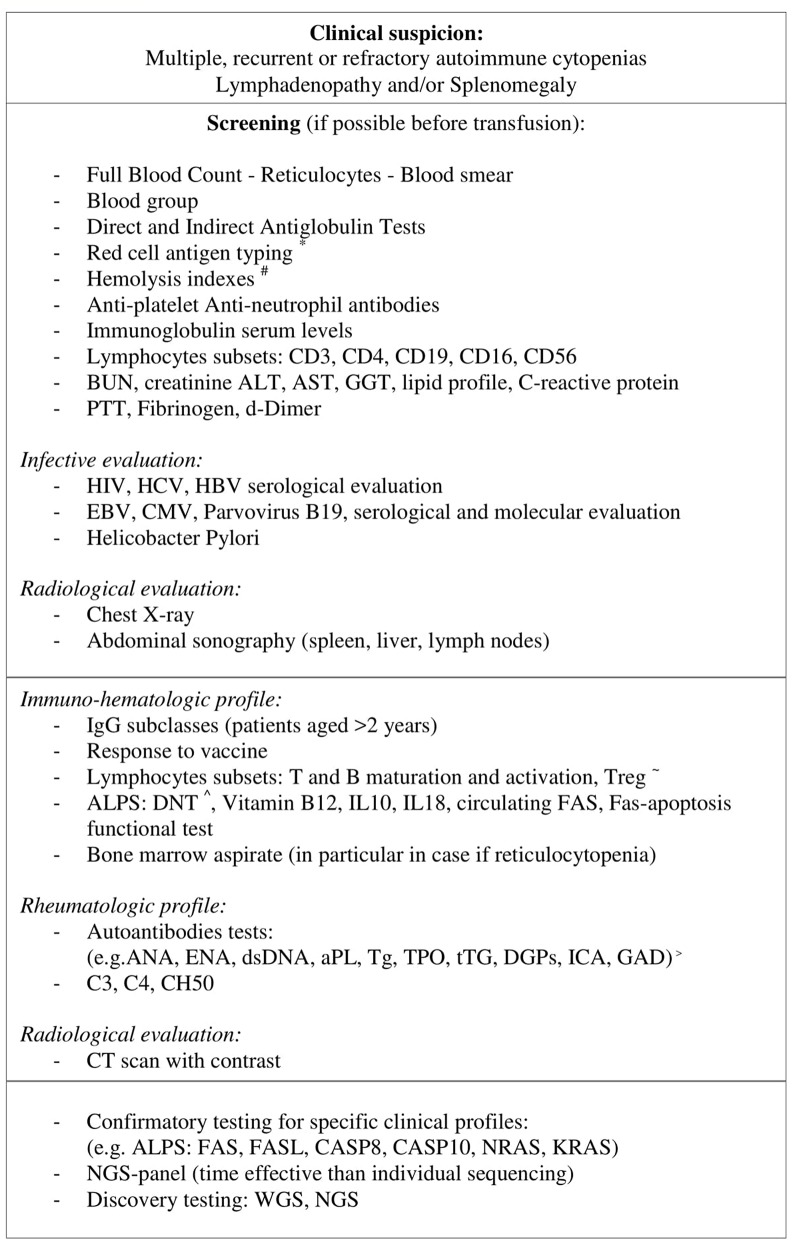
Evans syndrome (ES) is a rare but challenging condition, characterized by recurrent and refractory cytopenia episodes. Recent discoveries highlighted that an appropriate diagnostic workup is fundamental to identify an underlying immune dysregulation such as primary immunodeficiencies or a rheumatological disease. We hereby describe clinical features and laboratory results of 12 pediatric patients affected by ES referred to the Pediatric Onco-Hematology Unit of Bologna. Patients experienced a median of four acute episodes of cytopenia with 9 years as median age at the onset of symptoms. In 8/12 (67%) patients an underlying etiology, primary immunodeficiencies, or rheumatological disease was identified. In 4/12 children, other immune manifestations were associated (Thyroiditis, Celiac disease, Psoriasis, Vitiligo, Myositis, Membranoproliferative Glomerulonephritis). ES remained the primary diagnosis in four patients (33%). At a median follow-up time of 4 years, 5/12 (42%) patients revealed a chronic ITP, partially responsive to second line therapy. Immunoglobulin Replacement Therapy (IRT) was effective with a good hematological values control in three patients with a secondary ES (ALPS, CVID, and a patient with Rubinstein Taybi Syndrome and a progressive severe B cell deficiency with hypogammaglobulinemia). Our experience highlights that, in pediatric patients, ES is often only the first manifestation of an immunological or rheumatological disease, especially when cytopenias are persistent or resistant to therapy, with an early-onset or when are associated with lymphadenopathy.
Keywords: Evans syndrome; autoimmune disease; children; immune cytopenias; immunological characterization; primary immunodeficiency; refractory cytopenia; rheumatological disease.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources