

Effect of Electronic Prescribing Strategies on Medication Error and Harm in Hospital: a Systematic Review and Meta-analysis
- PMID: 31396810
- PMCID: PMC6816608
- DOI: 10.1007/s11606-019-05236-8
Effect of Electronic Prescribing Strategies on Medication Error and Harm in Hospital: a Systematic Review and Meta-analysis
Abstract
Background: Computerized physician order entry and clinical decision support systems are electronic prescribing strategies that are increasingly used to improve patient safety. Previous reviews show limited effect on patient outcomes. Our objective was to assess the impact of electronic prescribing strategies on medication errors and patient harm in hospitalized patients.
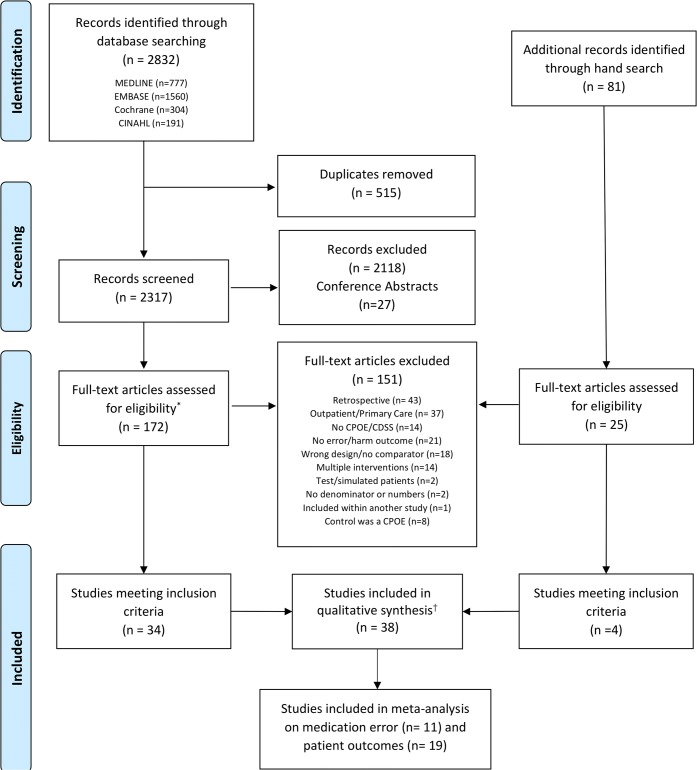
Methods: MEDLINE, EMBASE, CENTRAL, and CINAHL were searched from January 2007 to January 2018. We included prospective studies that compared hospital-based electronic prescribing strategies with control, and reported on medication error or patient harm. Data were abstracted by two reviewers and pooled using random effects model. Study quality was assessed using the Effective Practice and Organisation of Care and evidence quality was assessed using Grading of Recommendations Assessment, Development, and Evaluation.
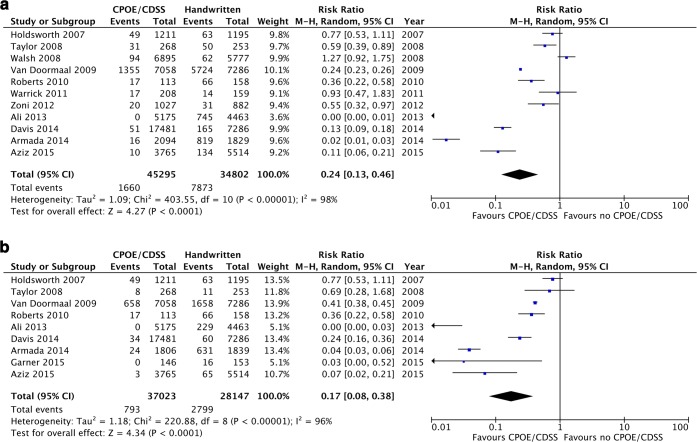
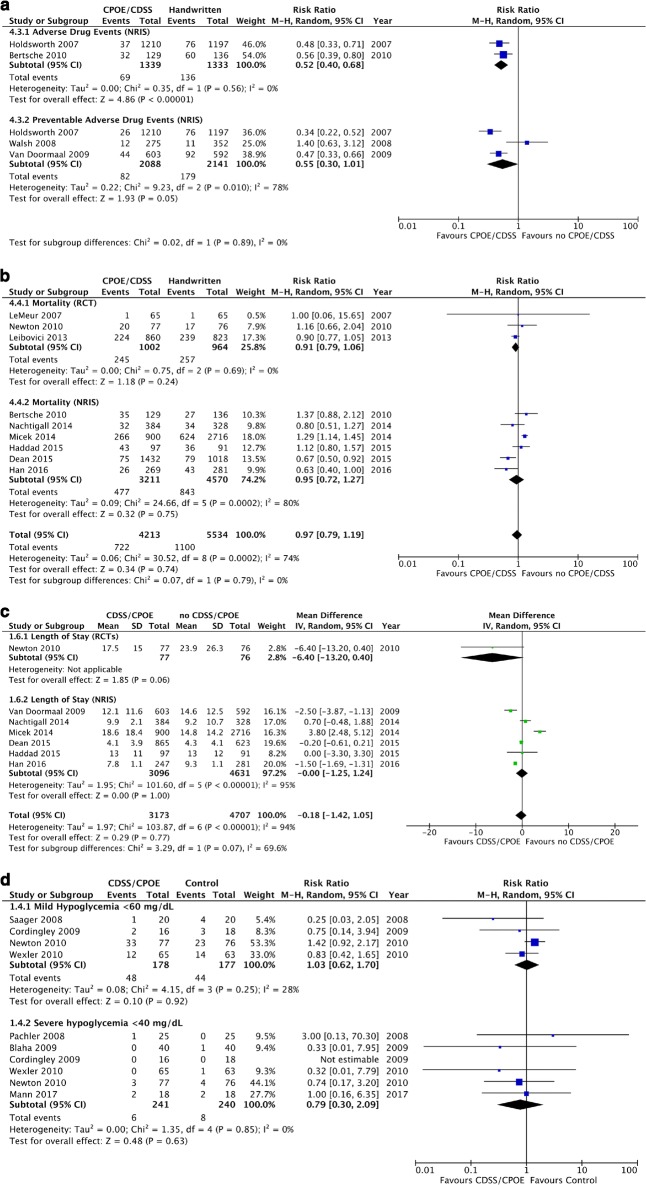
Results: Thirty-eight studies were included; comprised of 11 randomized control trials and 27 non-randomized interventional studies. Electronic prescribing strategies reduced medication errors (RR 0.24 (95% CI 0.13, 0.46), I2 98%, n = 11) and dosing errors (RR 0.17 (95% CI 0.08, 0.38), I2 96%, n = 9), with both risk ratios significantly affected by advancing year of publication. There was a significant effect of electronic prescribing strategies on adverse drug events (ADEs) (RR 0.52 (95% CI 0.40, 0.68), I2 0%, n = 2), but not on preventable ADEs (RR 0.55 (95% CI 0.30, 1.01), I2 78%, n = 3), hypoglycemia (RR 1.03 (95% CI 0.62-1.70), I2 28%, n = 7), length of stay (MD - 0.18 (95% - 1.42, 1.05), I2 94%, n = 7), or mortality (RR 0.97 (95% CI 0.79, 1.19), I2 74%, n = 9). The quality of evidence was rated very low.
Discussion: Electronic prescribing strategies decrease medication errors and adverse drug events, but had no effect on other patient outcomes. Conservative interpretations of these findings are supported by significant heterogeneity and the preponderance of low-quality studies.
Keywords: CDSS; CPOE; electronic prescribing; medication error; preventable adverse drug events.
Conflict of interest statement
N Roumeliotis has doctoral financial support from “Fonds de Recherche Quebec-Santé (FRQS)” as well as from the Canadian Critical Care Trials Group (CCCTG). The remaining authors have disclosed that they do not have any conflicts of interest.
Figures
References
-
- Crossing the Quality Chiasm . Crossing the Quality Chasm: A New Health System for the 21st Century. Washington DC: 2001 by the National Academy of Sciences; 2001.
-
- Miller Kristen, Mosby Danielle, Capan Muge, Kowalski Rebecca, Ratwani Raj, Noaiseh Yaman, Kraft Rachel, Schwartz Sanford, Weintraub William S, Arnold Ryan. Interface, information, interaction: a narrative review of design and functional requirements for clinical decision support. Journal of the American Medical Informatics Association. 2017;25(5):585–592. doi: 10.1093/jamia/ocx118. - DOI - PMC - PubMed
