

Cardiovascular Adverse Events Associated With BRAF and MEK Inhibitors: A Systematic Review and Meta-analysis
- PMID: 31397860
- PMCID: PMC6692687
- DOI: 10.1001/jamanetworkopen.2019.8890
Cardiovascular Adverse Events Associated With BRAF and MEK Inhibitors: A Systematic Review and Meta-analysis
Abstract
Importance: Cardiovascular adverse events (CVAEs) after treatment with BRAF and MEK inhibitors in patients with melanoma remain incompletely characterized.
Objective: To determine the association of BRAF and MEK inhibitor treatment with CVAEs in patients with melanoma compared with BRAF inhibitor monotherapy.
Data sources: PubMed, Cochrane, and Web of Science were systematically searched for keywords vemurafenib, dabrafenib, encorafenib, trametinib, binimetinib, and cobinimetinib from database inception through November 30, 2018.
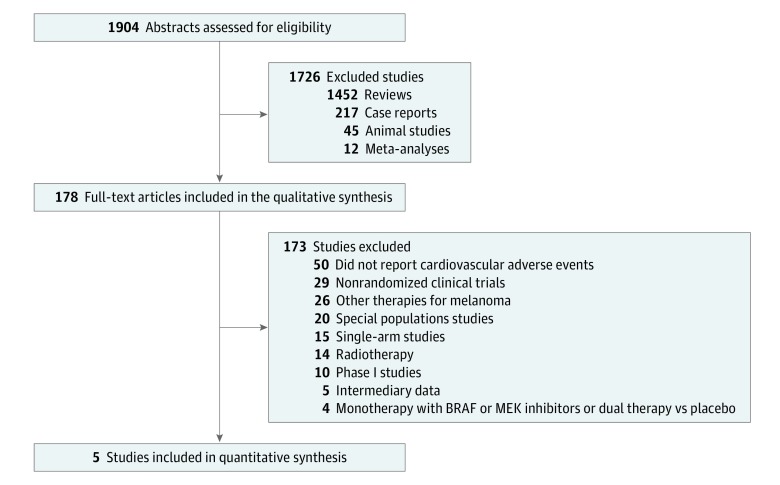
Study selection: Randomized clinical trials reporting on CVAEs in patients with melanoma being treated with BRAF and MEK inhibitors compared with patients with melanoma being treated with BRAF inhibitor monotherapy were selected.
Data extraction and synthesis: Data assessment followed the Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) guidelines. Pooled relative risks (RRs) and 95% CIs were determined using random-effects and fixed-effects analyses. Subgroup analyses were conducted to assess study-level characteristics associated with CVAEs.
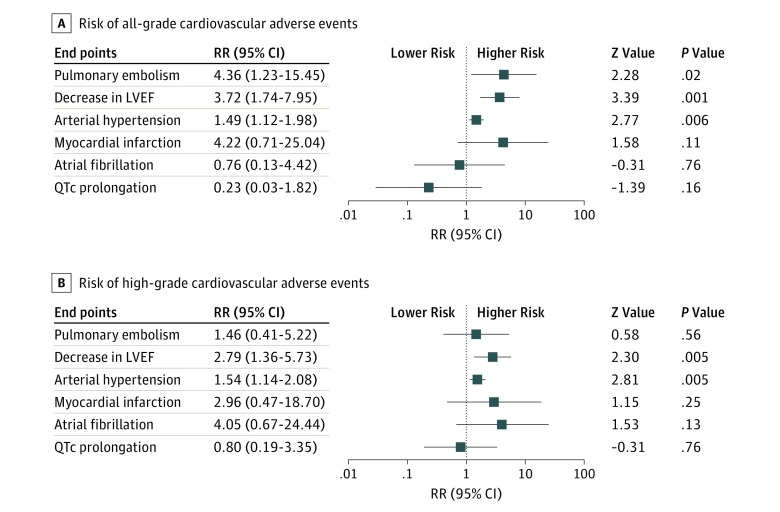
Main outcomes and measures: The selected end points were pulmonary embolism, a decrease in left ventricular ejection fraction, arterial hypertension, myocardial infarction, atrial fibrillation, and QTc interval prolongation. All-grade and high-grade (≥3) CVAEs were recorded.
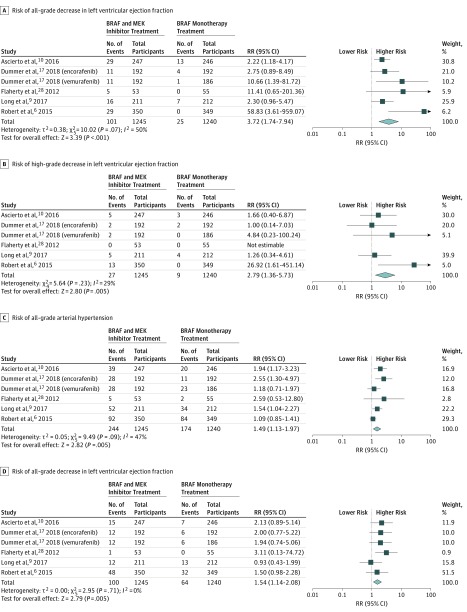
Results: Overall, 5 randomized clinical trials including 2317 patients with melanoma were selected. Treatment with BRAF and MEK inhibitors was associated with an increased risk of pulmonary embolism (RR, 4.36; 95% CI, 1.23-15.44; P = .02), a decrease in left ventricular ejection fraction (RR, 3.72; 95% CI, 1.74-7.94; P < .001), and arterial hypertension (RR, 1.49; 95% CI, 1.12-1.97; P = .005) compared with BRAF inhibitor monotherapy. The RRs for myocardial infarction, atrial fibrillation, and QTc prolongation were similar between the groups. These results were consistent when assessing high-grade CVAEs (left ventricular ejection fraction: RR, 2.79; 95% CI, 1.36-5.73; P = .005; I2 = 29%; high-grade arterial hypertension: RR, 1.54; 95% CI, 1.14-2.08; P = .005; I2 = 0%), but RRs for high-grade pulmonary embolism were similar between groups. A higher risk of a decrease in left ventricular ejection fraction was associated with patients with a mean age younger than 55 years (RR, 26.50; 95% CI, 3.58-196.10; P = .001), and the associated risk of pulmonary embolism was higher for patients with a mean follow-up time longer than 15 months (RR, 7.70; 95% CI, 1.40-42.12; P = .02).
Conclusions and relevance: Therapy with BRAF and MEK inhibitors was associated with a higher risk of CVAEs compared with BRAF inhibitor monotherapy. The findings may help to balance between beneficial melanoma treatment and cardiovascular morbidity and mortality.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
