

Comparison of Pheochromocytoma-Specific Morbidity and Mortality Among Adults With Bilateral Pheochromocytomas Undergoing Total Adrenalectomy vs Cortical-Sparing Adrenalectomy
- PMID: 31397861
- PMCID: PMC6692838
- DOI: 10.1001/jamanetworkopen.2019.8898
Comparison of Pheochromocytoma-Specific Morbidity and Mortality Among Adults With Bilateral Pheochromocytomas Undergoing Total Adrenalectomy vs Cortical-Sparing Adrenalectomy
Abstract
Importance: Large studies investigating long-term outcomes of patients with bilateral pheochromocytomas treated with either total or cortical-sparing adrenalectomies are needed to inform clinical management.
Objective: To determine the association of total vs cortical-sparing adrenalectomy with pheochromocytoma-specific mortality, the burden of primary adrenal insufficiency after bilateral adrenalectomy, and the risk of pheochromocytoma recurrence.
Design, setting, and participants: This cohort study used data from a multicenter consortium-based registry for 625 patients treated for bilateral pheochromocytomas between 1950 and 2018. Data were analyzed from September 1, 2018, to June 1, 2019.
Exposures: Total or cortical-sparing adrenalectomy.
Main outcomes and measures: Primary adrenal insufficiency, recurrent pheochromocytoma, and mortality.
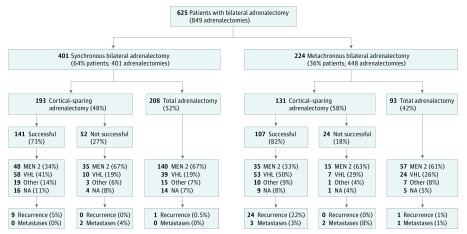
Results: Of 625 patients (300 [48%] female) with a median (interquartile range [IQR]) age of 30 (22-40) years at diagnosis, 401 (64%) were diagnosed with synchronous bilateral pheochromocytomas and 224 (36%) were diagnosed with metachronous pheochromocytomas (median [IQR] interval to second adrenalectomy, 6 [1-13] years). In 505 of 526 tested patients (96%), germline mutations were detected in the genes RET (282 patients [54%]), VHL (184 patients [35%]), and other genes (39 patients [7%]). Of 849 adrenalectomies performed in 625 patients, 324 (52%) were planned as cortical sparing and were successful in 248 of 324 patients (76.5%). Primary adrenal insufficiency occurred in all patients treated with total adrenalectomy but only in 23.5% of patients treated with attempted cortical-sparing adrenalectomy. A third of patients with adrenal insufficiency developed complications, such as adrenal crisis or iatrogenic Cushing syndrome. Of 377 patients who became steroid dependent, 67 (18%) developed at least 1 adrenal crisis and 50 (13%) developed iatrogenic Cushing syndrome during median (IQR) follow-up of 8 (3-25) years. Two patients developed recurrent pheochromocytoma in the adrenal bed despite total adrenalectomy. In contrast, 33 patients (13%) treated with successful cortical-sparing adrenalectomy developed another pheochromocytoma within the remnant adrenal after a median (IQR) of 8 (4-13) years, all of which were successfully treated with another surgery. Cortical-sparing surgery was not associated with survival. Overall survival was associated with comorbidities unrelated to pheochromocytoma: of 63 patients who died, only 3 (5%) died of metastatic pheochromocytoma.
Conclusions and relevance: Patients undergoing cortical-sparing adrenalectomy did not demonstrate decreased survival, despite development of recurrent pheochromocytoma in 13%. Cortical-sparing adrenalectomy should be considered in all patients with hereditary pheochromocytoma.
Conflict of interest statement
Figures
References
-
- Lloyd RV, Osamura R, Klöppel G, Rosai J, eds. WHO Classifiaction of Tumours of Endocrine Organs. 4th ed Lyon, France: IARC Publications; 2017.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
