

Progress towards lymphatic filariasis elimination in Ghana from 2000-2016: Analysis of microfilaria prevalence data from 430 communities
- PMID: 31398203
- PMCID: PMC6709921
- DOI: 10.1371/journal.pntd.0007115
Progress towards lymphatic filariasis elimination in Ghana from 2000-2016: Analysis of microfilaria prevalence data from 430 communities
Abstract
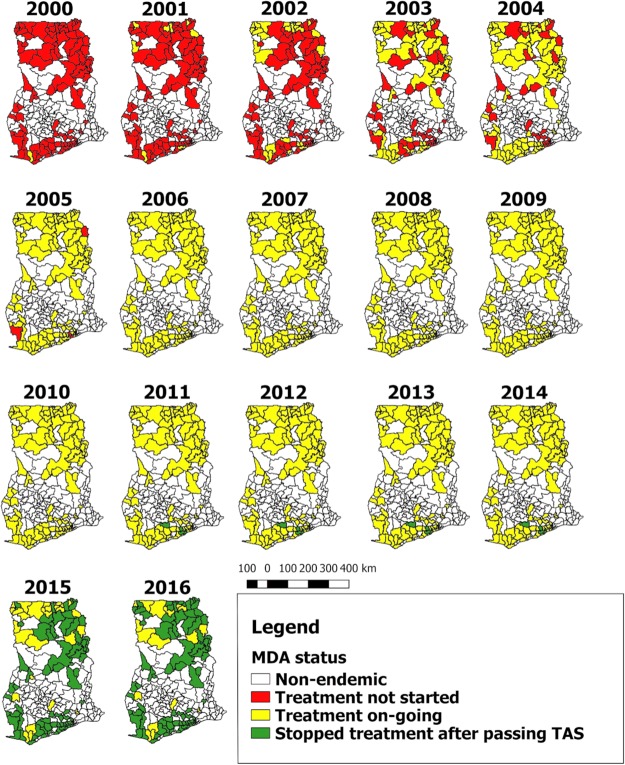
Background: Ghana started its national programme to eliminate lymphatic filariasis (LF) in 2000, with mass drug administration (MDA) with ivermectin and albendazole as main strategy. We review the progress towards elimination that was made by 2016 for all endemic districts of Ghana and analyze microfilaria (mf) prevalence from sentinel and spot-check sites in endemic districts.
Methods: We reviewed district level data on the history of MDA and outcomes of transmission assessment surveys (TAS). We further collated and analyzed mf prevalence data from sentinel and spot-check sites.
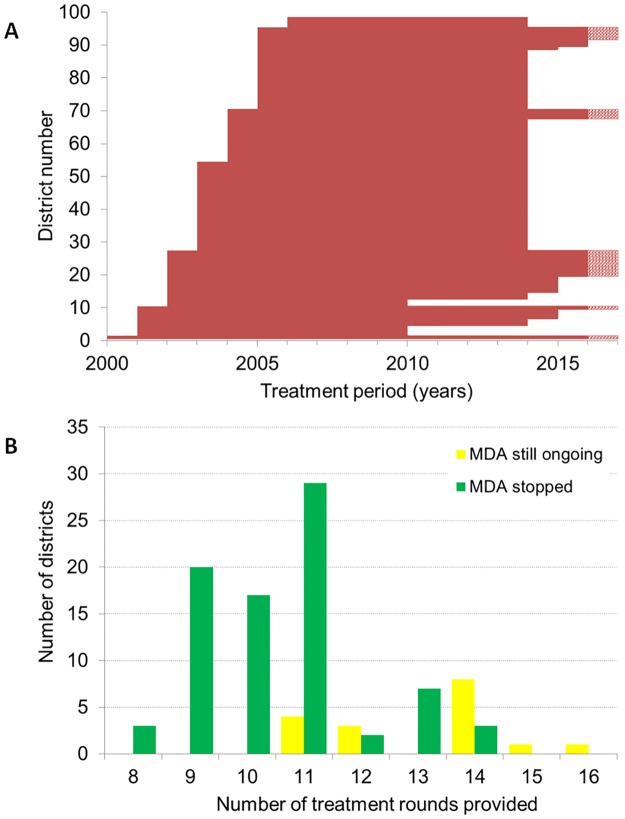
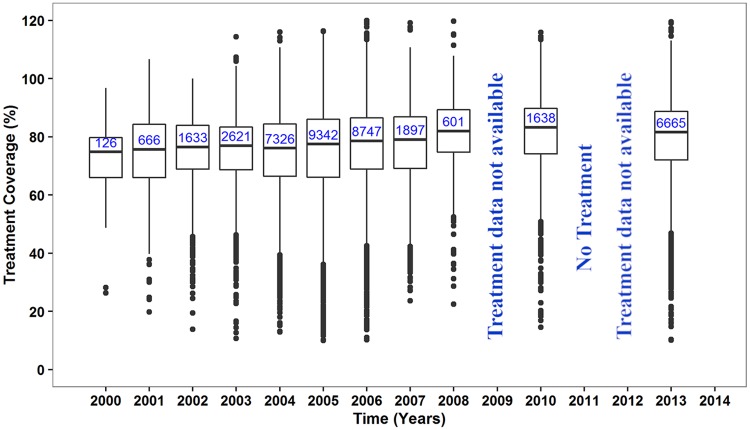
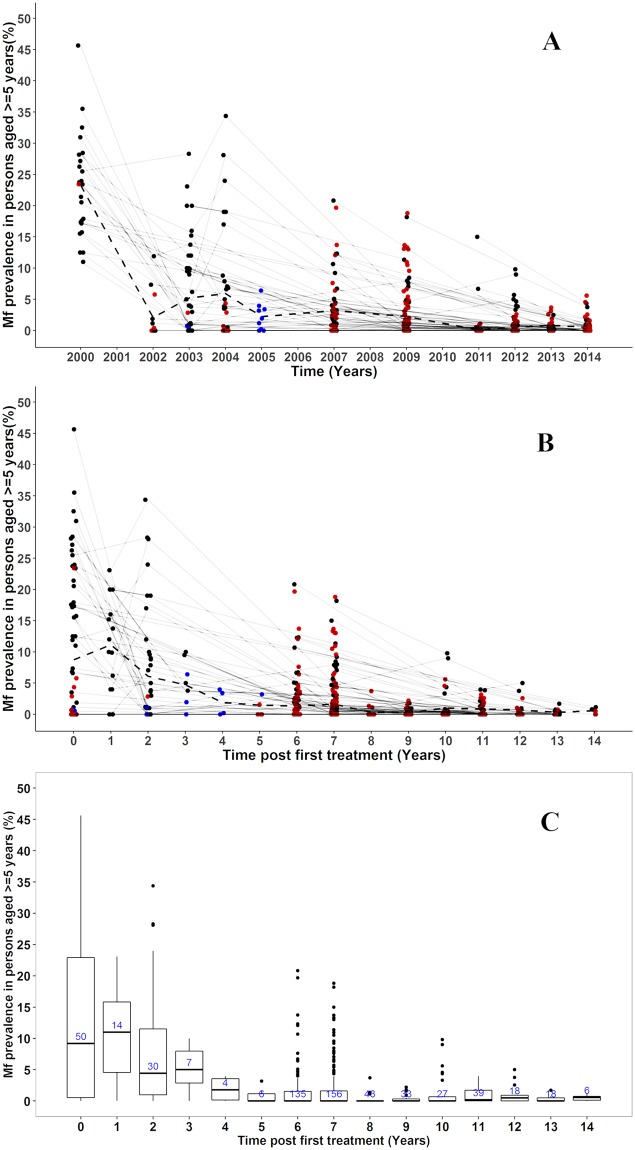
Results: MDA was initiated in 2001-2006 in all 98 endemic districts; by the end of 2016, 81 had stopped MDA after passing TAS and after an average of 11 rounds of treatment (range 8-14 rounds). The median reported coverage for the communities was 77-80%. Mf prevalence survey data were available for 430 communities from 78/98 endemic districts. Baseline mf prevalence data were available for 53 communities, with an average mf prevalence of 8.7% (0-45.7%). Repeated measurements were available for 78 communities, showing a steep decrease in mean mf prevalence in the first few years of MDA, followed by a gradual further decline. In the 2013 and 2014 surveys, 7 and 10 communities respectively were identified with mf prevalence still above 1% (maximum 5.6%). Fifteen of the communities above threshold are all within districts where MDA was still ongoing by 2016.
Conclusions: The MDA programme of the Ghana Health Services has reduced mf prevalence in sentinel sites below the 1% threshold in 81/98 endemic districts in Ghana, yet 15 communities within 13 districts (MDA ongoing by 2016) had higher prevalence than this threshold during the surveys in 2013 and 2014. These districts may need to intensify interventions to achieve the WHO 2020 target.
Conflict of interest statement
Authors have declared they have no competing interests exists.
Figures
References
-
- Michael E, Bundy DA, Grenfell BT (1996) Re-assessing the global prevalence and distribution of lymphatic filariasis. Parasitology 112 (Pt 4): 409–428. - PubMed
-
- WHO (2015) Global programme to eliminate lymphatic filariasis: progress report, 2014. Wkly Epidemiol Rec 90: 489–504. - PubMed
-
- Ottesen EA (2000) The global programme to eliminate lymphatic filariasis. Trop Med Int Health 5: 591–594. - PubMed
-
- WHO (2017) Summary of global update on preventive chemotherapy implementation in 2016: crossing the billion. Weekly epidemiological records 40: 589–608. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
