

Tumor Microbiome Diversity and Composition Influence Pancreatic Cancer Outcomes
- PMID: 31398337
- PMCID: PMC7288240
- DOI: 10.1016/j.cell.2019.07.008
Tumor Microbiome Diversity and Composition Influence Pancreatic Cancer Outcomes
Abstract
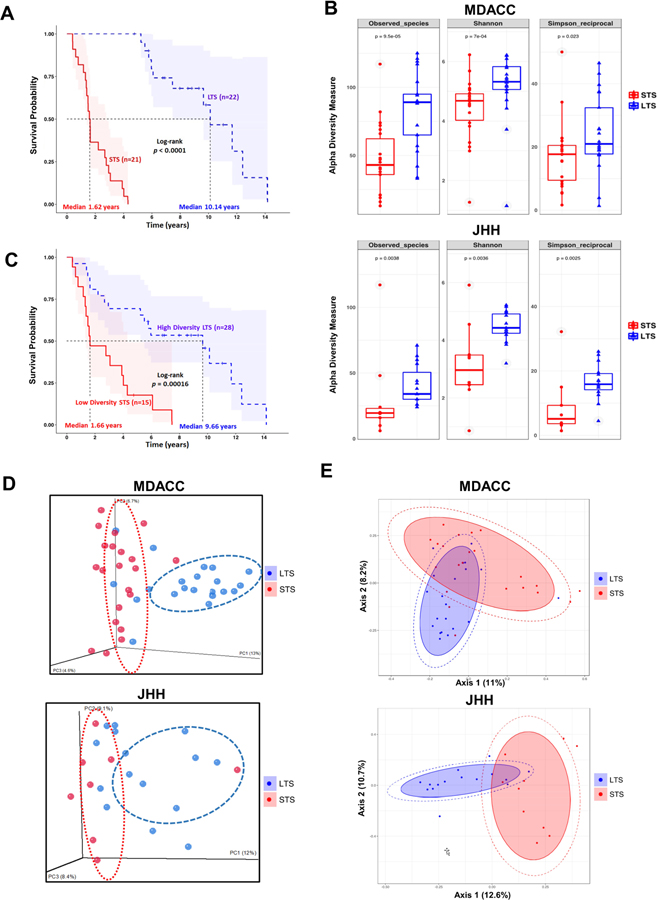
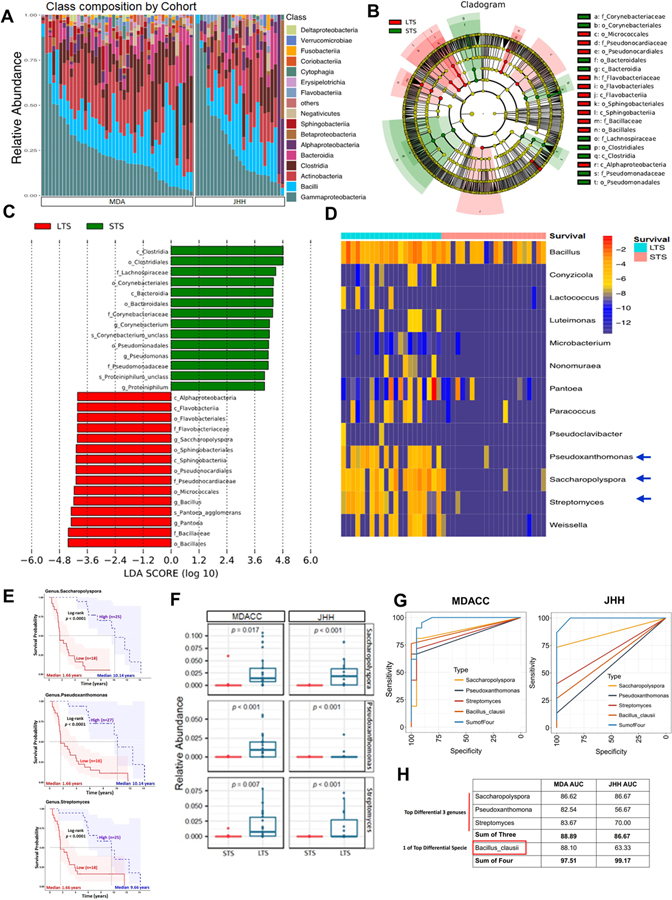
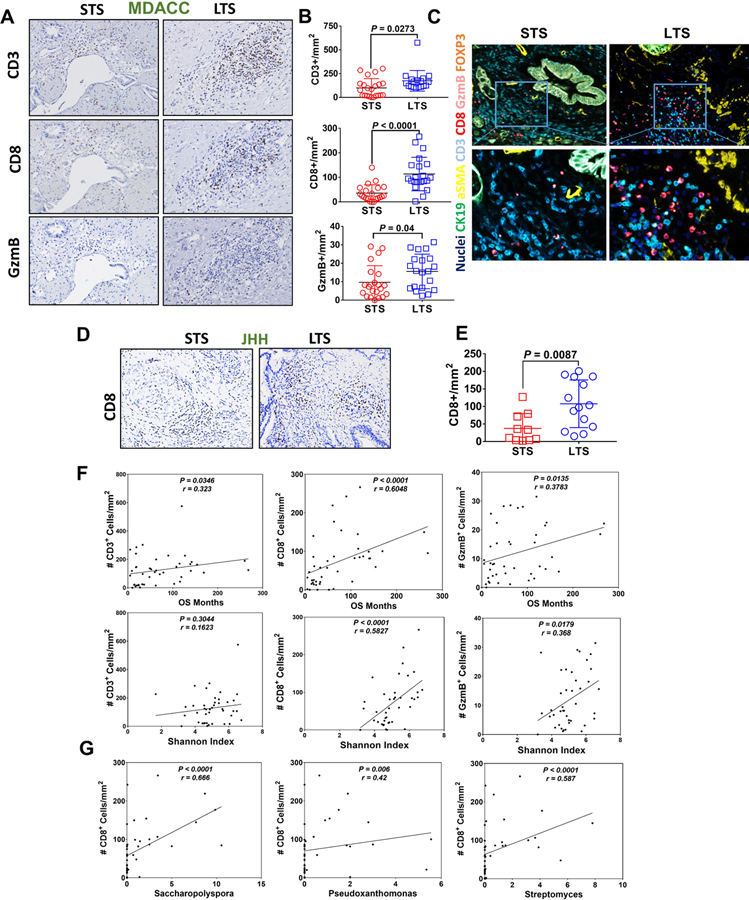
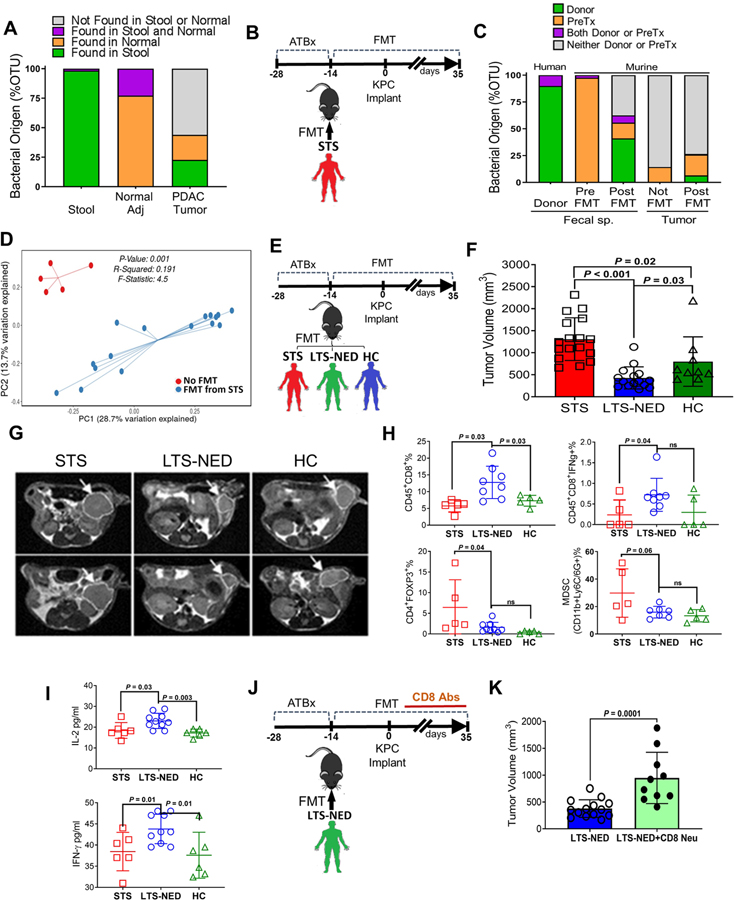
Most patients diagnosed with resected pancreatic adenocarcinoma (PDAC) survive less than 5 years, but a minor subset survives longer. Here, we dissect the role of the tumor microbiota and the immune system in influencing long-term survival. Using 16S rRNA gene sequencing, we analyzed the tumor microbiome composition in PDAC patients with short-term survival (STS) and long-term survival (LTS). We found higher alpha-diversity in the tumor microbiome of LTS patients and identified an intra-tumoral microbiome signature (Pseudoxanthomonas-Streptomyces-Saccharopolyspora-Bacillus clausii) highly predictive of long-term survivorship in both discovery and validation cohorts. Through human-into-mice fecal microbiota transplantation (FMT) experiments from STS, LTS, or control donors, we were able to differentially modulate the tumor microbiome and affect tumor growth as well as tumor immune infiltration. Our study demonstrates that PDAC microbiome composition, which cross-talks to the gut microbiome, influences the host immune response and natural history of the disease.
Keywords: CD8; PDAC; antibiotics; cancer survivors; fecal microbial transplants; immunoactivation; microbiota; pancreatic cancer; tumor microbiome.
Published by Elsevier Inc.
Conflict of interest statement
Figures
Comment in
-
Tumour microbiome defines outcomes.Nat Rev Cancer. 2019 Oct;19(10):545. doi: 10.1038/s41568-019-0201-1. Nat Rev Cancer. 2019. PMID: 31471581 No abstract available.
-
Tumour microbiome defines outcomes.Nat Rev Gastroenterol Hepatol. 2019 Nov;16(11):649. doi: 10.1038/s41575-019-0208-9. Nat Rev Gastroenterol Hepatol. 2019. PMID: 31477872 No abstract available.
-
Microbes as biomarkers and targets in pancreatic cancer.Nat Rev Clin Oncol. 2019 Nov;16(11):665-666. doi: 10.1038/s41571-019-0276-3. Nat Rev Clin Oncol. 2019. PMID: 31530941 No abstract available.
References
-
- Atarashi K, Tanoue T, Oshima K, Suda W, Nagano Y, Nishikawa H, Fukuda S, Saito T, Narushima S, Hase K, et al. (2013). Treg induction by a rationally selected mixture of Clostridia strains from the human microbiota. Nature 500, 232–236. - PubMed
-
- Benjamini Y, Drai D, Elmer G, Kafkafi N, and Golani I(2001). Controlling the false discovery rate in behavior genetics research. Behav Brain Res 125, 279–284. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
