

Growing a new human kidney
- PMID: 31399199
- PMCID: PMC6856720
- DOI: 10.1016/j.kint.2019.04.040
Growing a new human kidney
Abstract
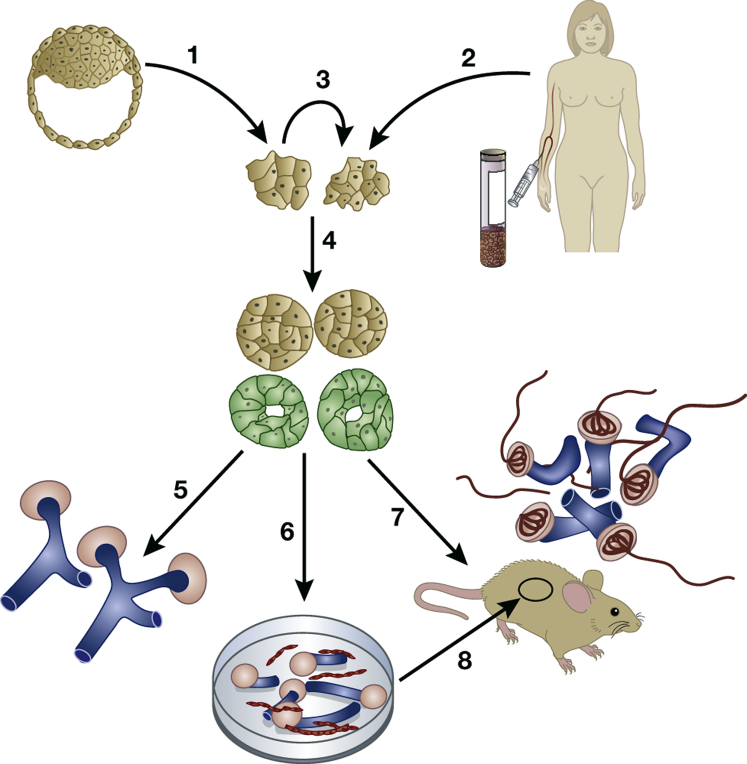
There are 3 reasons to generate a new human kidney. The first is to learn more about the biology of the developing and mature organ. The second is to generate tissues with which to model congenital and acquired kidney diseases. In particular, growing human kidneys in this manner ultimately should help us understand the mechanisms of common chronic kidney diseases such as diabetic nephropathy and others featuring fibrosis, as well as nephrotoxicity. The third reason is to provide functional kidney tissues that can be used directly in regenerative medicine therapies. The second and third reasons to grow new human kidneys are especially compelling given the millions of persons worldwide whose lives depend on a functioning kidney transplant or long-term dialysis, as well as those with end-stage renal disease who die prematurely because they are unable to access these treatments. As shown in this review, the aim to create healthy human kidney tissues has been partially realized. Moreover, the technology shows promise in terms of modeling genetic disease. In contrast, barely the first steps have been taken toward modeling nongenetic chronic kidney diseases or using newly grown human kidney tissue for regenerative medicine therapies.
Keywords: disease; gene; mesonephros; metanephros; organoid; regeneration; stem cell.
Crown Copyright © 2019. Published by Elsevier Inc. All rights reserved.
Figures


References
-
- Vize P.D., Woolf A.S., Bard J.B.L. Elsevier Science/Academic Press; Cambridge, MA: 2003. The Kidney: From Normal Development to Congenital Abnormalities.
-
- Liyanage T., Ninomiya T., Jha V. Worldwide access to treatment for end-stage kidney disease: a systematic review. Lancet. 2015;385:1975–1982. - PubMed
-
- Osathanondh V., Potter E.L. Development of human kidney as shown by microdissection. III. Formation and interrelationship of collecting tubules and nephrons. Arch Pathol. 1963;76:290–302. - PubMed
-
- Osathanondh V., Potter E.L. Development of human kidney as shown by microdissection. II. Renal pelvis, calyces, and papillae. Arch Pathol. 1963;76:277–289. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
