

Clinicopathologic subtype of Alzheimer's disease presenting as corticobasal syndrome
- PMID: 31399334
- PMCID: PMC9262170
- DOI: 10.1016/j.jalz.2019.04.011
Clinicopathologic subtype of Alzheimer's disease presenting as corticobasal syndrome
Abstract
Introduction: The corticobasal syndrome (CBS) is associated with several neuropathologic disorders, including corticobasal degeneration and Alzheimer's disease (AD).
Method: In this report, we studied 43 AD patients with CBS (AD-CBS) and compared them with 42 AD patients with typical amnestic syndrome (AD-AS), as well as 15 cases of corticobasal degeneration and CBS pathology.
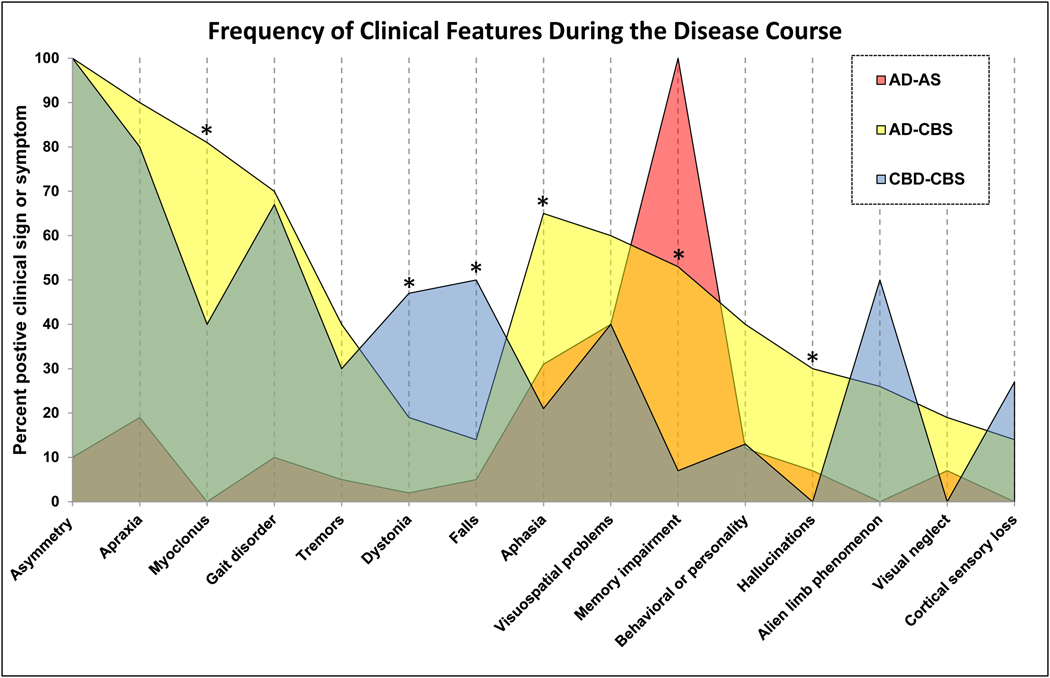
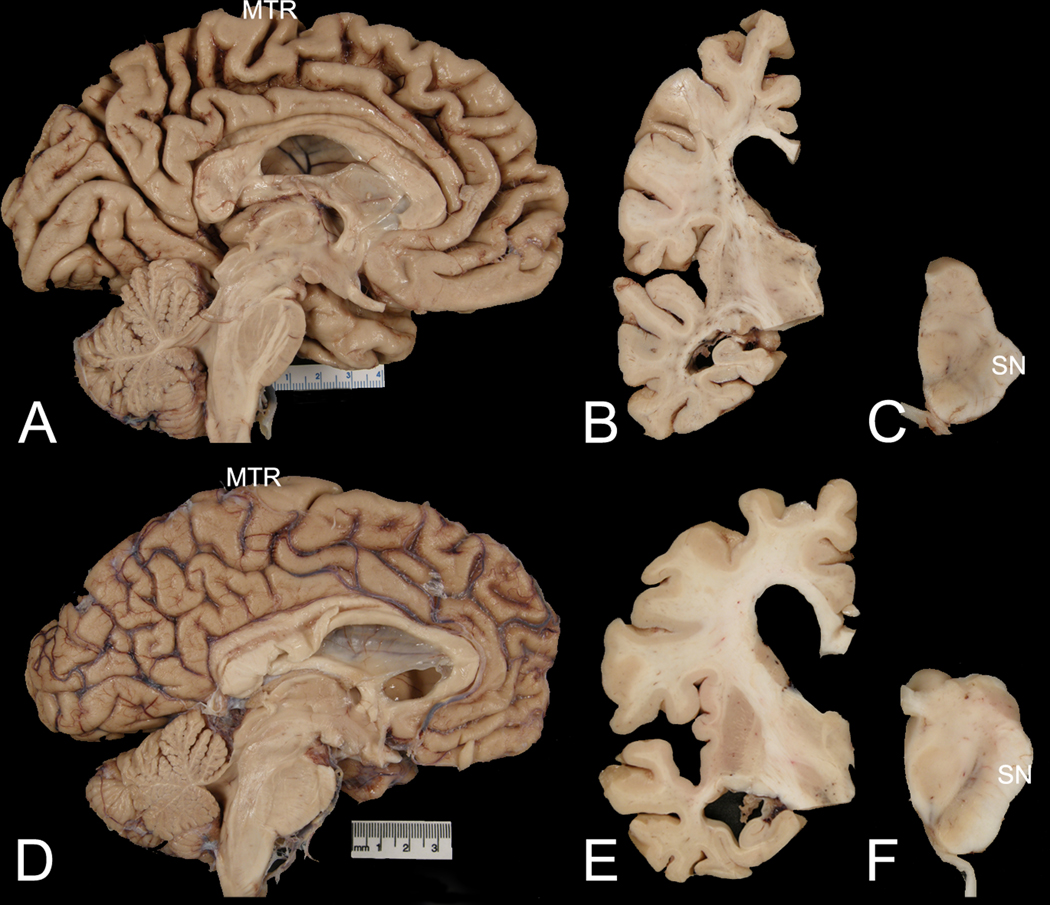
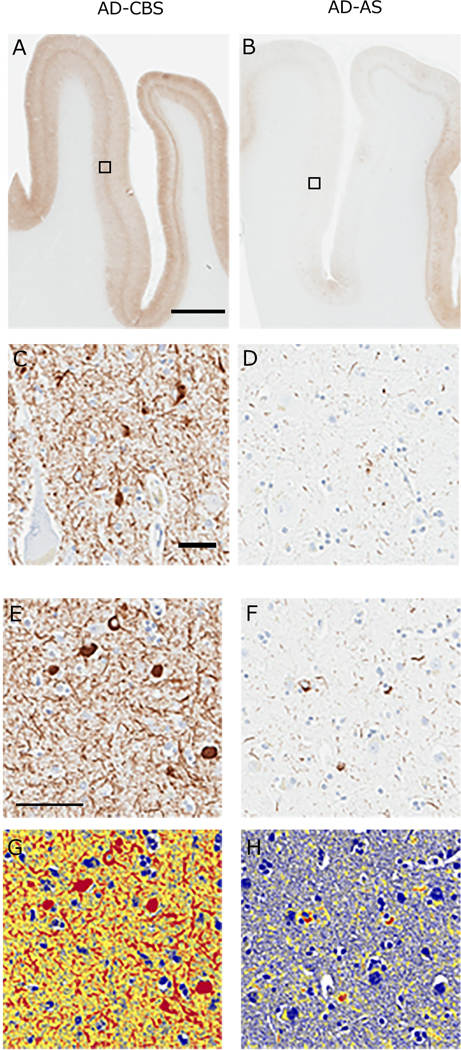
Results: Unlike AD-AS, AD-CBS had prominent motor problems, including limb apraxia (90%), myoclonus (81%), and gait disorders (70%). Alien limb phenomenon was reported in 26% and cortical sensory loss in 14%. Language problems were also more frequent in AD-CBS, and memory impairment was less frequent. AD-CBS had more tau pathology in perirolandic cortices but less in superior temporal cortex than AD-AS. In addition, AD-CBS had greater neuronal loss in the substantia nigra.
Discussion: AD-CBS is a clinicopathological subtype of AD with an atypical distribution of Alzheimer-type tau pathology. Greater neuronal loss in the substantia nigra may contribute to Parkinsonism which is not a feature of typical AD.
Keywords: Alzheimer's disease; Corticobasal syndrome; Neurodegeneration; Neuropathology; Tau.
Copyright © 2019. Published by Elsevier Inc.
Conflict of interest statement
Conflict of interest statement: The authors have declared that no conflict of interest exists.
Figures
References
-
- Dubois B, Feldman HH, Jacova C, Hampel H, Molinuevo JL, Blennow K, et al. Advancing research diagnostic criteria for Alzheimer’s disease: the IWG-2 criteria. Lancet Neurol. 2014;13:614–29. - PubMed
-
- Panegyres PK, Goh J, McCarthy M, Campbell AI. The Nature and Natural History of Posterior Cortical Atrophy Syndrome: A Variant of Early-onset Alzheimer Disease. Alzheimer Dis Assoc Disord. 2017;31:295–306. - PubMed
-
- Johnson JK, Head E, Kim R, Starr A, Cotman CW. Clinical and pathological evidence for a frontal variant of Alzheimer disease. Arch Neurol. 1999;56:1233–9. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
