

Is inspiratory muscle training (IMT) an acceptable treatment option for people with chronic obstructive pulmonary disease (COPD) who have declined pulmonary rehabilitation (PR) and can IMT enhance PR uptake? A single-group prepost feasibility study in a home-based setting
- PMID: 31399454
- PMCID: PMC6701573
- DOI: 10.1136/bmjopen-2018-028507
Is inspiratory muscle training (IMT) an acceptable treatment option for people with chronic obstructive pulmonary disease (COPD) who have declined pulmonary rehabilitation (PR) and can IMT enhance PR uptake? A single-group prepost feasibility study in a home-based setting
Abstract
Objectives: This feasibility study aimed to assess the acceptability of inspiratory muscle training (IMT) in people with chronic obstructive pulmonary disease (COPD) who declined pulmonary rehabilitation (PR) as a potential treatment option or precursor to PR. Objectives were to assess attitudes to IMT, PR and alternatives to PR; factors influencing adherence with IMT and acceptability of outcome measures, research tools and study protocol.
Design: A pragmatic, mixed methods, prepost feasibility study was conducted. Recruitment took place over a 4-month period. Participants were followed up for a period of 6 months.
Settings: IMT sessions and assessments were conducted in the domiciliary setting.
Participants: Inclusion criteria: people over the age of 35, stable COPD, Medical Research Council Dyspnoea scale of 3 or above, declined PR.
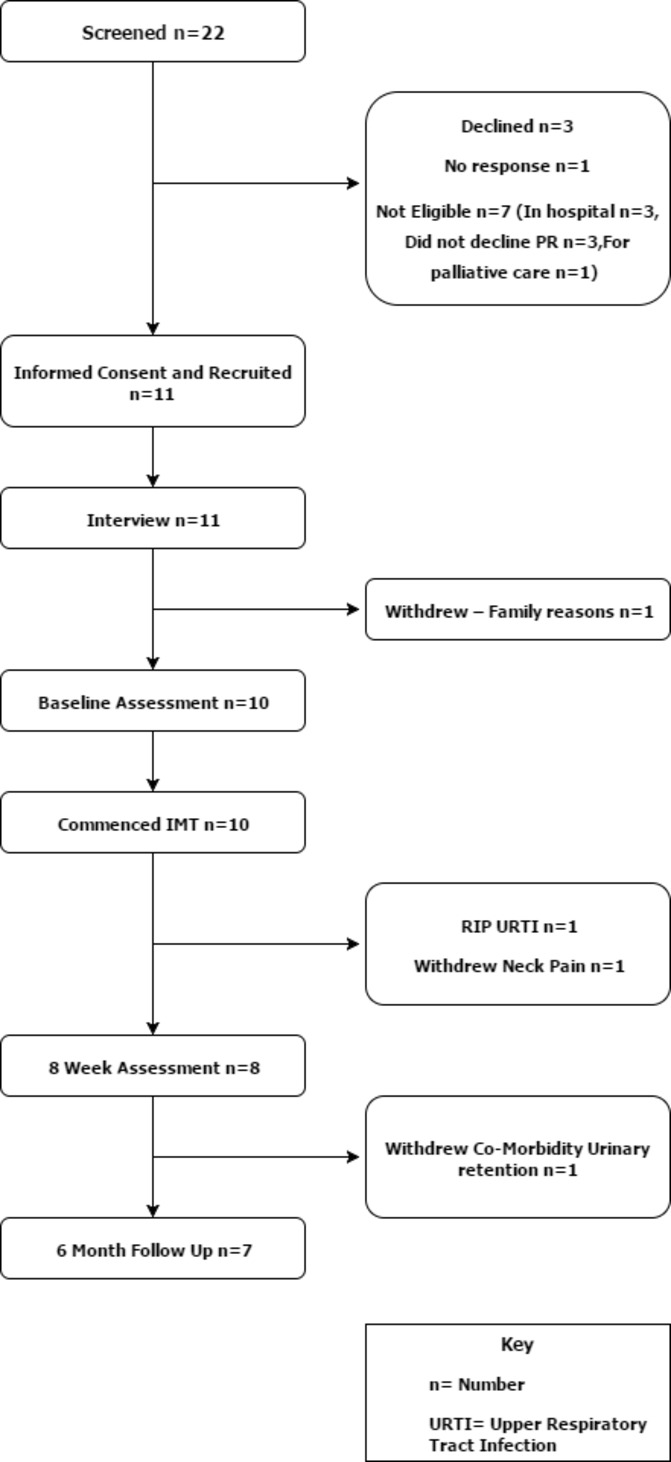
Exclusion criteria: history of spontaneous pneumothorax, incomplete recovery from a traumatic pneumothorax, asthma, known recently perforated eardrum, unstable angina, ventricular dysrhythmias, cerebrovascular event or myocardial infarction within the last 2 months. Participants were selected from a purposive sample. Of the 22 potential participants screened, 11 were recruited and interviewed. Ten participants commenced IMT. Seven participants completed the follow-up assessment.
Intervention: Eight weeks of IMT twice a day, 5 days a week with visits once weekly by a physiotherapist. Unsupervised IMT twice a day three times a week until follow-up at 6 months.
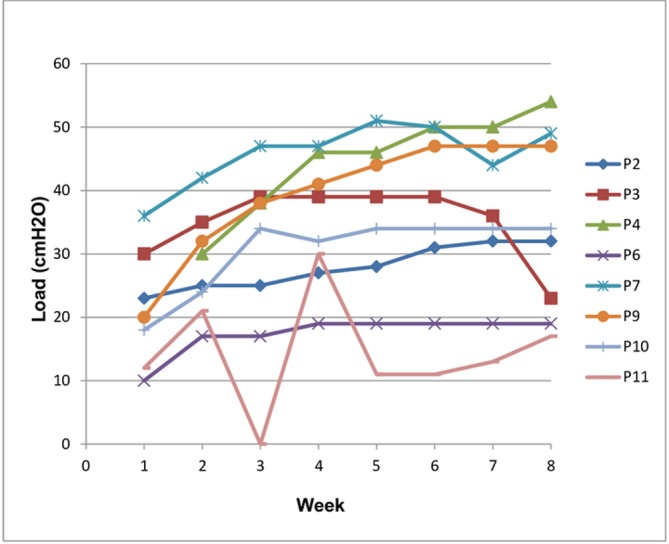
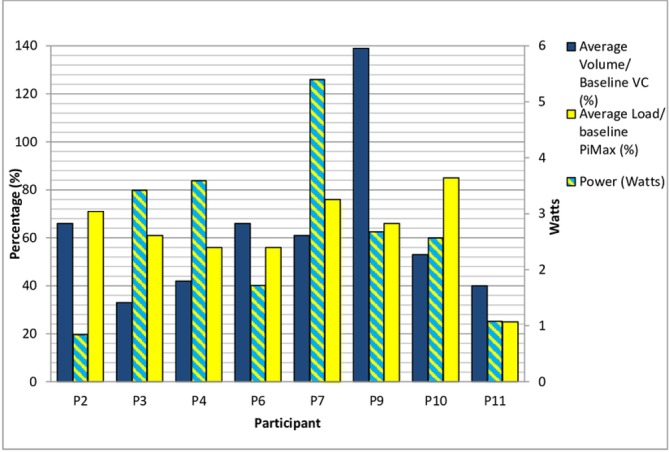
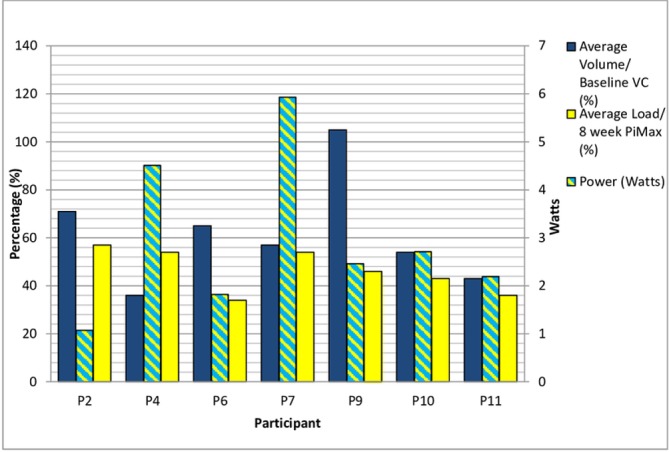
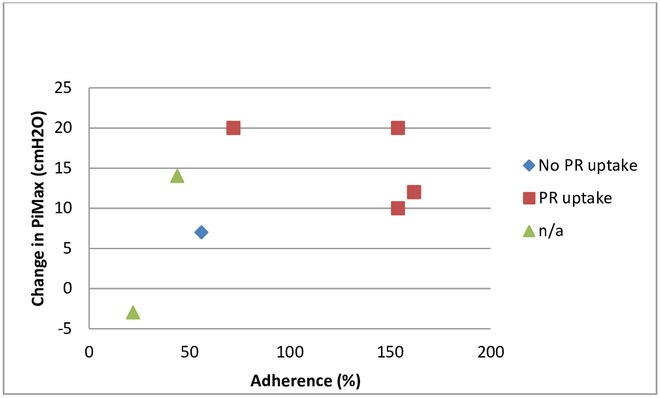
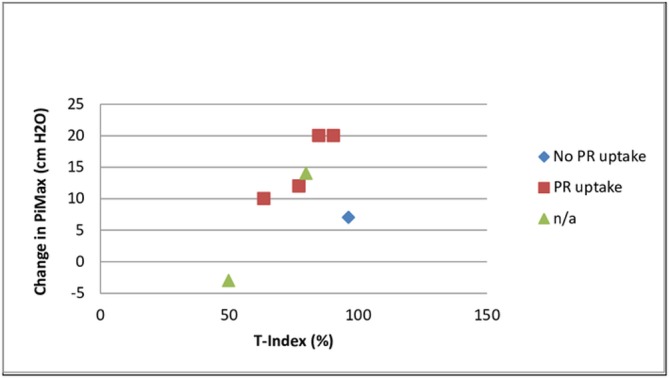
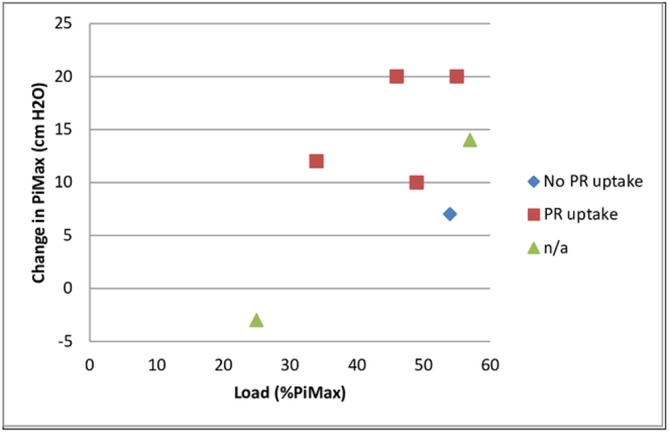
Outcomes: Acceptability of IMT and the study process was explored via semi-structured interviews. Adherence with IMT was assessed by the Powerbreathe K3 device and participant diaries. Uptake of PR was identified.
Results: IMT was found to be acceptable. Adherence was explored. Four people went on to participate in PR.
Conclusions: Feasibility was established. A randomised controlled trial is warranted to establish efficacy and cost-effectiveness of IMT in those who decline PR and IMT as an intervention to promote uptake of PR.
Trial registration number: NCT01956565; Post-results.
Keywords: adherence; chronic airways disease; inspiratory muscle training; pulmonary rehabilitation; rehabilitation medicine; uptake.
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- NICE. Chronic obstructive pulmonary disease: management of chronic obstructive pulmonary disease in adults in primary and secondary care: National Clinical Guideline Centre, 2010.
-
- Steiner M. Pulmonary Rehabilitation: Time to breathe better. National Chronic Obstructive Pulmonary Disease (COPD) Audit Programme: Resources and organisation of Pulmonary Rehabilitation services in England and Wales 2015, 2015.
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials