

Acetabular Lateral View: Effective Fluoroscopic Imaging to Evaluate Screw Penetration Intraoperatively
- PMID: 31399554
- PMCID: PMC6699199
- DOI: 10.12659/MSM.915906
Acetabular Lateral View: Effective Fluoroscopic Imaging to Evaluate Screw Penetration Intraoperatively
Abstract
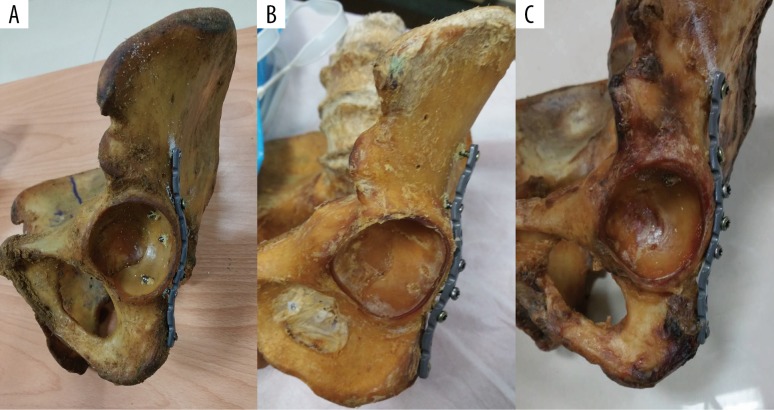
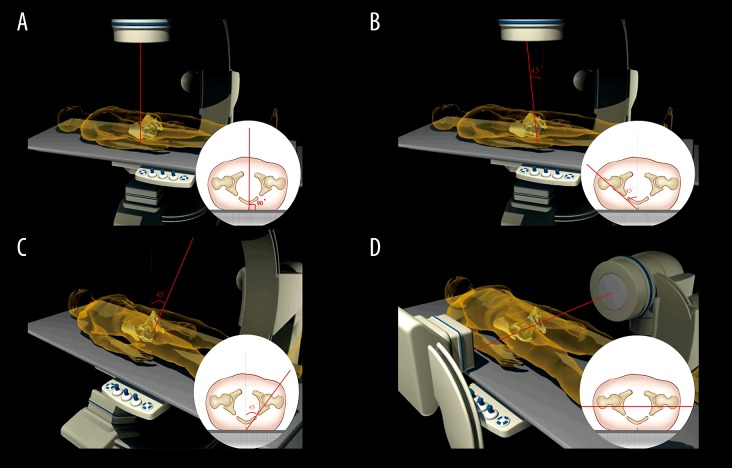
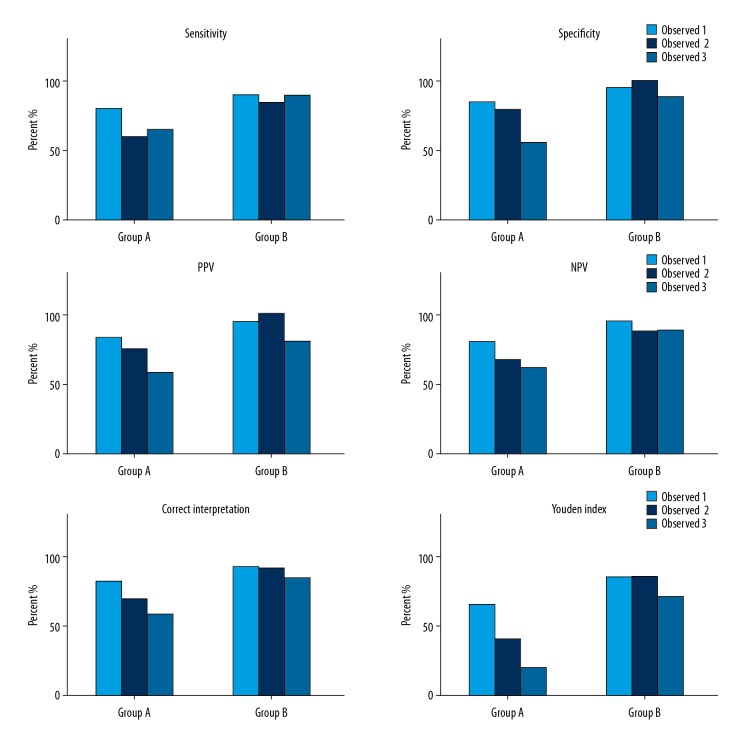
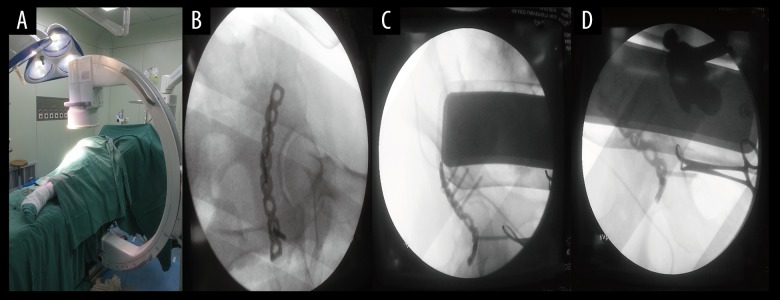
BACKGROUND Screw penetration into the hip joint is a severe complication during acetabular fracture surgery. The standard fluoroscopic views of the pelvis cannot provide adequate safety during screw insertion. The aim of this research was to determine and evaluate the accuracy of the acetabular lateral view for screw placement. MATERIAL AND METHODS Twenty screws were randomly chosen and intentionally penetrated into the articular surface (1-2 mm), and the remaining 20 screws were extra-articular ones positioned in close proximity to the articular surface. Three surgeons, each evaluating 40 screws, provided a total of 120 rated observations for each screw position. We compared the traditional view or combined with lateral acetabular view with the criterion standard based on unaided visual assessment. A blinded and independent review of each pelvic intraoperative fluoroscopy was made by 3 independent observers. Specificity, sensitivity, positive predictive value, negative predictive value, correct interpretation, intra-class correlation coefficients (ICC), and Youden index were calculated. RESULTS There were significant differences in sensitivity, NPV, correct interpretation, and Youden index between the 2 groups (P<0.05). The ICC was 0.531 when the antero-posterior, iliac, and obturator oblique views were used. The ICC was remarkably increased when using a combination of the ''lateral'' view and the standard views for screw perforation of the joint. CONCLUSIONS Use of the lateral view of the acetabulum can be a complementary method to identify malpositioned screws, and it helps increase the accuracy rate of inserting screws in the treatment of posterior wall fracture.
Figures

References
-
- Moed BR, WillsonCarr SE, Watson JT. Results of operative treatment of fractures of the posterior wall of the acetabulum. J Bone Joint Surg Am. 2002;84-A:752–58. - PubMed
-
- Archdeacon MT, Dailey SK. Efficacy of routine postoperative CT scan after open reduction and internal fixation of the acetabulum. J Orthop Trauma. 2015;29:354–58. - PubMed
-
- Kendoff D, Gardner MJ, Citak M, et al. Value of 3D fluoroscopic imaging of acetabular fractures comparison to 2D fluoroscopy and CT imaging. Arch Orthop Trauma Surg. 2008;128:599–605. - PubMed
-
- Carmack DB, Moed BR, McCarroll K, Freccero D. Accuracy of detecting screw penetration of the acetabulum with intraoperative fluoroscopy and computed tomography. J Bone Joint Surg Am. 2001;83-A:1370–75. - PubMed
-
- Norris BL, Hahn DH, Bosse MJ, et al. Intraoperative fluoroscopy to evaluate fracture reduction and hardware placement during acetabular surgery. J Orthop Trauma. 1999;13:414–17. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
