

Pheochromocytoma- and paraganglioma-triggered Takotsubo syndrome
- PMID: 31399912
- PMCID: PMC6717601
- DOI: 10.1007/s12020-019-02035-3
Pheochromocytoma- and paraganglioma-triggered Takotsubo syndrome
Abstract
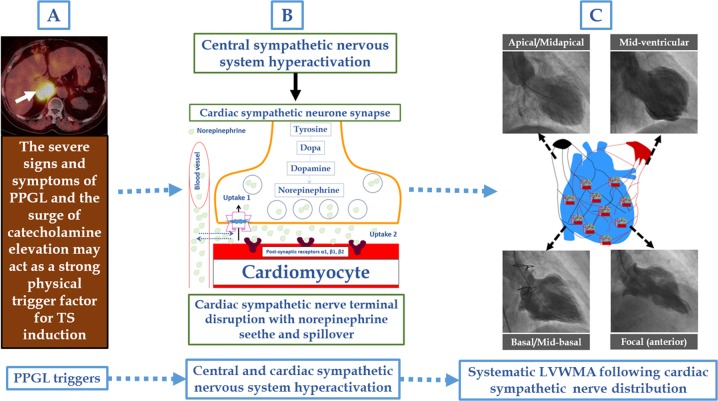
Takotsubo syndrome (TS), also known as neurogenic stunned myocardium or broken heart syndrome, is a recognized acute cardiac syndrome. In about 70% of cases, the syndrome is preceded by an emotional or a physical stressor. Among the innumerable physical trigger factors that may induce TS are pheochromocytomas and paragangliomas (PPGLs). PPGL-associated cardiovascular complications as "myocarditis", "myocardial infarction", "reversible cardiomyopathies", and "transient repolarization electrocardiographic changes" have been described since more than 70 years. During the last two decades, dozens of cases of PPGL-induced TS have been reported. PPGLs display increased catecholamine levels, sometimes massively elevated, which may trigger TS, most likely through hyperactivation of sympathetic nervous system including the cardiac sympathetic nerve terminal disruption with norepinephrine seethe and spillover. PPGL-induced TS is characterized by a dramatic clinical presentation with hemodynamic compromise and high complication rates. The prevalence of global and apical sparing pattern of TS in PPGL-induced TS is significantly higher than in other TS populations. In this report, the associations of PPGL-induced cardiovascular complications are analyzed, and clinical features, complications, outcome and treatment of PPGL-induced TS are reviewed.
Keywords: Broken heart; Catecholamine; Myocardial stunning; Paraganglioma; Pheochromocytoma; Takotsubo.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures
References
-
- Amar L, Servais A, Gimenez-Roqueplo AP, Zinzindohoue F, Chatellier G, Plouin PF. Year of diagnosis, features at presentation, and risk of recurrence in patients with pheochromocytoma or secreting paraganglioma. J. Clin. Endocrinol. Metab. 2005;90(4):2110–2116. doi: 10.1210/jc.2004-1398. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
