

Clinical exome sequencing vs. usual care for hereditary colorectal cancer diagnosis: A pilot comparative effectiveness study
- PMID: 31400517
- PMCID: PMC6741782
- DOI: 10.1016/j.cct.2019.105820
Clinical exome sequencing vs. usual care for hereditary colorectal cancer diagnosis: A pilot comparative effectiveness study
Abstract
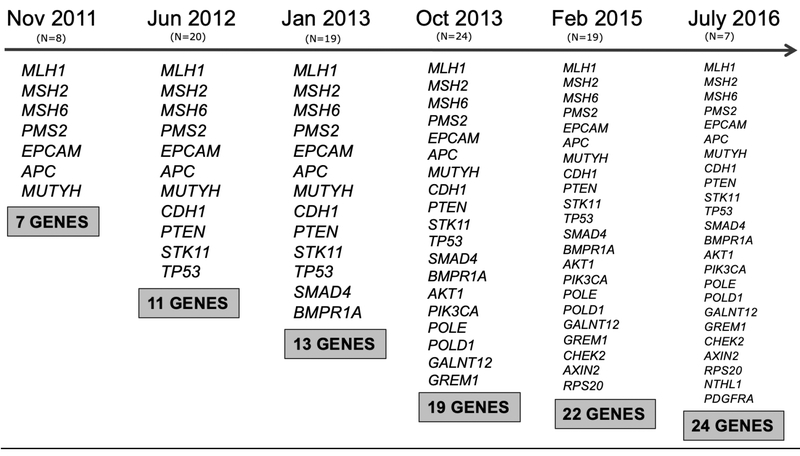
Background: Clinical exome sequencing (CES) provides the advantage of assessing genetic variation across the human exome compared to a traditional stepwise diagnostic approach or multi-gene panels. Comparative effectiveness research methods offer an approach to better understand the patient-centered and economic outcomes of CES.
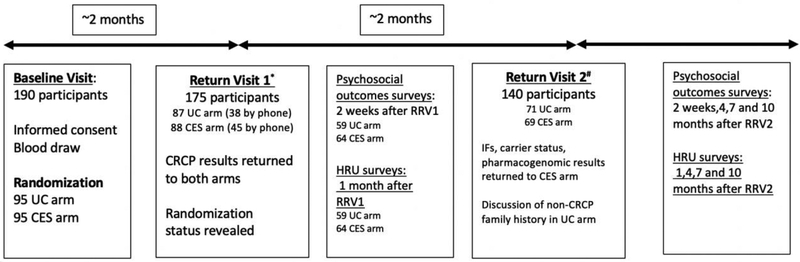
Purpose: To evaluate CES compared to usual care (UC) in the diagnostic work-up of inherited colorectal cancer/polyposis (CRCP) in a randomized controlled trial (RCT).
Methods: The primary outcome was clinical sensitivity for the diagnosis of inherited CRCP; secondary outcomes included psychosocial outcomes, family communication, and healthcare resource utilization. Participants were surveyed 2 and 4 weeks after results return and at 3-month intervals up to 1 year.
Results: Evolving outcome measures and standard of care presented critical challenges. The majority of participants in the UC arm received multi-gene panels [94.73%]. Rates of genetic findings supporting the diagnosis of hereditary CRCP were 7.5% [7/93] vs. 5.4% [5/93] in the CES and UC arms, respectively (P = 0.28). Differences in privacy concerns after receiving CRCP results were identified (0.88 in UC vs 0.38 in CES, P = 0.05); however, healthcare resource utilization, family communication and psychosocial outcomes were similar between the two arms. More participants with positive results (17.7%) intended to change their life insurance 1 month after the first return visit compared to participants returned a variant of uncertain significance (9.1%) or negative result (4.8%) (P = 0.09).
Conclusion: Our results suggest that CES provides similar clinical benefits to multi-gene panels in the diagnosis of hereditary CRCP.
Keywords: Clinical exome sequencing; Comparative effectiveness; Hereditary colorectal cancer/polyposis.
Copyright © 2019 Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
References
-
- Giardiello FM, Allen JI, Axilbund JE, Boland CR, Burke CA, Burt RW, et al. Guidelines on genetic evaluation and management of lynch syndrome: A consensus statement by the us multi-society task force on colorectal cancer. Gastroenterology 2014;147:502–26. doi: 10.1053/j.gastro.2014.04.001. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
