

Bronchoalveolar lavage cytokines are of minor value to diagnose complications following lung transplantation
- PMID: 31400641
- PMCID: PMC7128992
- DOI: 10.1016/j.cyto.2019.154794
Bronchoalveolar lavage cytokines are of minor value to diagnose complications following lung transplantation
Abstract
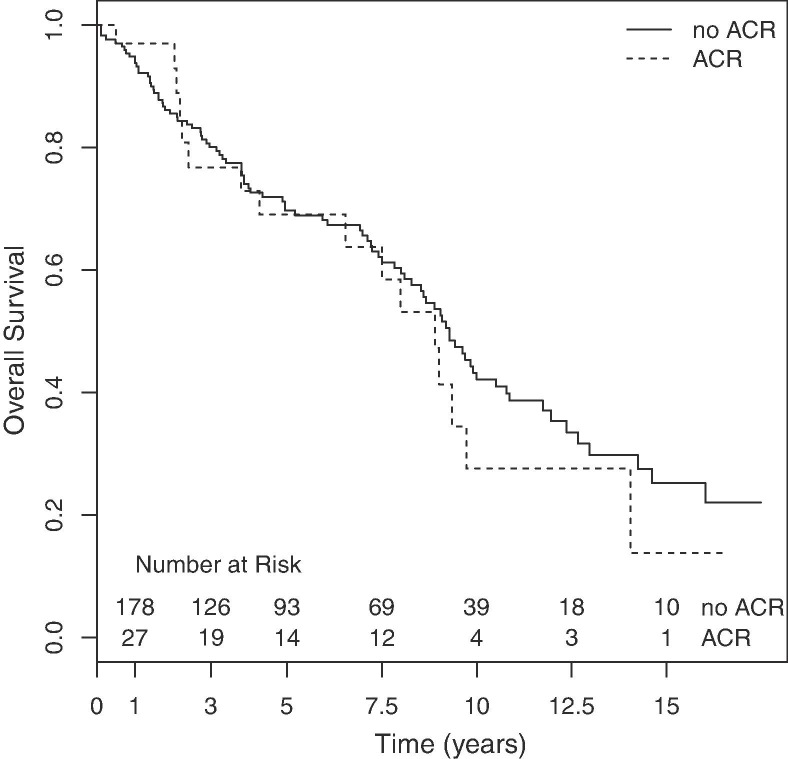
Early diagnosis and treatment of acute cellular rejection (ACR) may improve long-term outcome for lung transplant recipients (LTRs). Cytokines have become valuable diagnostic tools in many medical fields. The role of bronchoalveolar lavage (BAL) cytokines is of unknown value to diagnose ACR and distinguish rejection from infection. We hypothesized that distinct cytokine patterns obtained by surveillance bronchoscopies during the first year after transplantation are associated with ACR and microbiologic findings. We retrospectively analyzed data from 319 patients undergoing lung transplantation at University Hospital Zurich from 1998 to 2016. We compared levels of IL-6, IL-8, IFN-γ and TNF-α in 747 BAL samples with transbronchial biopsies (TBB) and microbiologic results from surveillance bronchoscopies. We aimed to define reference values that would allow distinction between four specific groups "ACR", "infection", "combined ACR and infection" and "no pathologic process". No definitive pattern was identified. Given the overlap between groups, these four cytokines are not suitable diagnostic markers for ACR or infection after lung transplantation.
Keywords: Acute cellular rejection; Bronchoalveolar lavage; Cytokine; Diagnosis; Lung transplantation; Standardization.
Copyright © 2019 Elsevier Ltd. All rights reserved.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures


References
-
- Chambers D.C., Yusen R.D., Cherikh W.S., et al. The registry of the international society for heart and lung transplantation: thirty-fourth adult lung and heart-lung transplantation report-2017; focus theme: allograft ischemic time. J. Heart Lung Transplant. 2017 - PubMed
-
- Swanson S.J., Mentzer S.J., Reilly J.J., et al. Surveillance transbronchial lung biopsies: implication for survival after lung transplantation. J. Thorac. Cardiovasc. Surg. 2000;119:27–37. - PubMed
-
- Khalifah A.P., Hachem R.R., Chakinala M.M., et al. Minimal acute rejection after lung transplantation: a risk for bronchiolitis obliterans syndrome. Am. J. Transplant. 2005;5:2022–2030. - PubMed
-
- Hachem R.R., Khalifah A.P., Chakinala M.M., et al. The significance of a single episode of minimal acute rejection after lung transplantation. Transplantation. 2005;80:1406–1413. - PubMed
-
- Sharples L.D., McNeil K., Stewart S., Wallwork J. Risk factors for bronchiolitis obliterans: a systematic review of recent publications. J Heart Lung Transplant. 2002;21:271–281. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
