

RESTORE-IMI 1: A Multicenter, Randomized, Double-blind Trial Comparing Efficacy and Safety of Imipenem/Relebactam vs Colistin Plus Imipenem in Patients With Imipenem-nonsusceptible Bacterial Infections
- PMID: 31400759
- PMCID: PMC7156774
- DOI: 10.1093/cid/ciz530
RESTORE-IMI 1: A Multicenter, Randomized, Double-blind Trial Comparing Efficacy and Safety of Imipenem/Relebactam vs Colistin Plus Imipenem in Patients With Imipenem-nonsusceptible Bacterial Infections
Abstract
Background: The β-lactamase inhibitor relebactam can restore imipenem activity against imipenem-nonsusceptible gram-negative pathogens. We evaluated imipenem/relebactam for treating imipenem-nonsusceptible infections.
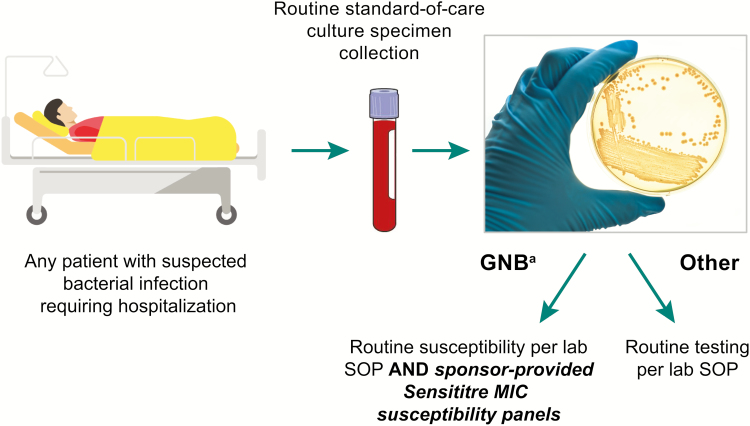
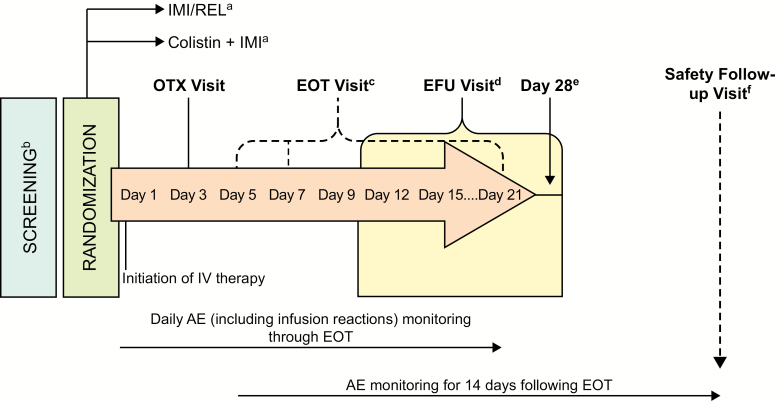
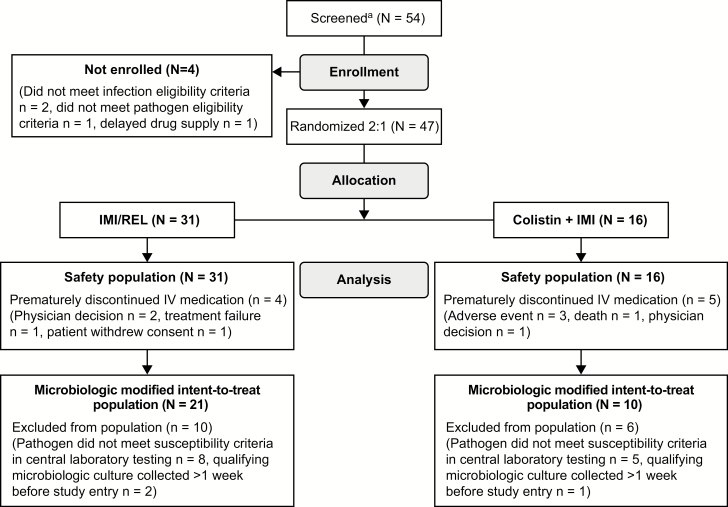
Methods: Randomized, controlled, double-blind, phase 3 trial. Hospitalized patients with hospital-acquired/ventilator-associated pneumonia, complicated intraabdominal infection, or complicated urinary tract infection caused by imipenem-nonsusceptible (but colistin- and imipenem/relebactam-susceptible) pathogens were randomized 2:1 to 5-21 days imipenem/relebactam or colistin+imipenem. Primary endpoint: favorable overall response (defined by relevant endpoints for each infection type) in the modified microbiologic intent-to-treat (mMITT) population (qualifying baseline pathogen and ≥1 dose study treatment). Secondary endpoints: clinical response, all-cause mortality, and treatment-emergent nephrotoxicity. Safety analyses included patients with ≥1 dose study treatment.
Results: Thirty-one patients received imipenem/relebactam and 16 colistin+imipenem. Among mITT patients (n = 21 imipenem/relebactam, n = 10 colistin+imipenem), 29% had Acute Physiology and Chronic Health Evaluation II scores >15, 23% had creatinine clearance <60 mL/min, and 35% were aged ≥65 years. Qualifying baseline pathogens: Pseudomonas aeruginosa (77%), Klebsiella spp. (16%), other Enterobacteriaceae (6%). Favorable overall response was observed in 71% imipenem/relebactam and 70% colistin+imipenem patients (90% confidence interval [CI] for difference, -27.5, 21.4), day 28 favorable clinical response in 71% and 40% (90% CI, 1.3, 51.5), and 28-day mortality in 10% and 30% (90% CI, -46.4, 6.7), respectively. Serious adverse events (AEs) occurred in 10% of imipenem/relebactam and 31% of colistin+imipenem patients, drug-related AEs in 16% and 31% (no drug-related deaths), and treatment-emergent nephrotoxicity in 10% and 56% (P = .002), respectively.
Conclusions: Imipenem/relebactam is an efficacious and well-tolerated treatment option for carbapenem-nonsusceptible infections.
Clinical trials registration: NCT02452047.
Keywords: KPC; cIAI; cUTI; carbapenem resistant; nosocomial pneumonia.
© The Author(s) 2019. Published by Oxford University Press for the Infectious Diseases Society of America.
Figures
Comment in
-
Reply to Sfeir.Clin Infect Dis. 2021 Apr 26;72(8):1485-1486. doi: 10.1093/cid/ciaa881. Clin Infect Dis. 2021. PMID: 32634242 No abstract available.
-
Imipenem-relebactam for Treatment of Carbapenem-resistant Gram-negative Bacteria: Where Do We Stand on In Vitro Susceptibility Testing?Clin Infect Dis. 2021 Apr 26;72(8):1484-1485. doi: 10.1093/cid/ciaa878. Clin Infect Dis. 2021. PMID: 32634243 No abstract available.
References
-
- Centers for Disease Control and Prevention. Antibiotic resistance threats in the United States, 2013. Available at: http://www.cdc.gov/drugresistance/threat-report-2013/. Accessed 3 June 2019.
-
- Cerceo E, Deitelzweig SB, Sherman BM, Amin AN. Multidrug-resistant gram-negative bacterial infections in the hospital setting: overview, implications for clinical practice, and emerging treatment options. Microb Drug Resist 2016; 22:412–31. - PubMed
-
- World Health Organization. Global priority list of antibiotic-resistant bacteria to guide research, discovery, and development of new antibiotics. 2017. Available at: https://www.who.int/medicines/publications/global-priority-list-antibiot...
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
