

Health, not weight loss, focused programmes versus conventional weight loss programmes for cardiovascular risk factors: a systematic review and meta-analysis
- PMID: 31400767
- PMCID: PMC6689181
- DOI: 10.1186/s13643-019-1083-8
Health, not weight loss, focused programmes versus conventional weight loss programmes for cardiovascular risk factors: a systematic review and meta-analysis
Abstract
Background: Obesity is a cardiovascular disease risk factor. Conventional weight loss (CWL) programmes focus on weight loss, however 'health, not weight loss, focused' (HNWL) programmes concentrate on improved health and well-being, irrespective of weight loss. What are the differences in CVD risk outcomes between these programmes?
Aim: To conduct a systematic review and meta-analysis to compare the effects of HNWL with CWL programmes on cardiovascular disease risk factors.
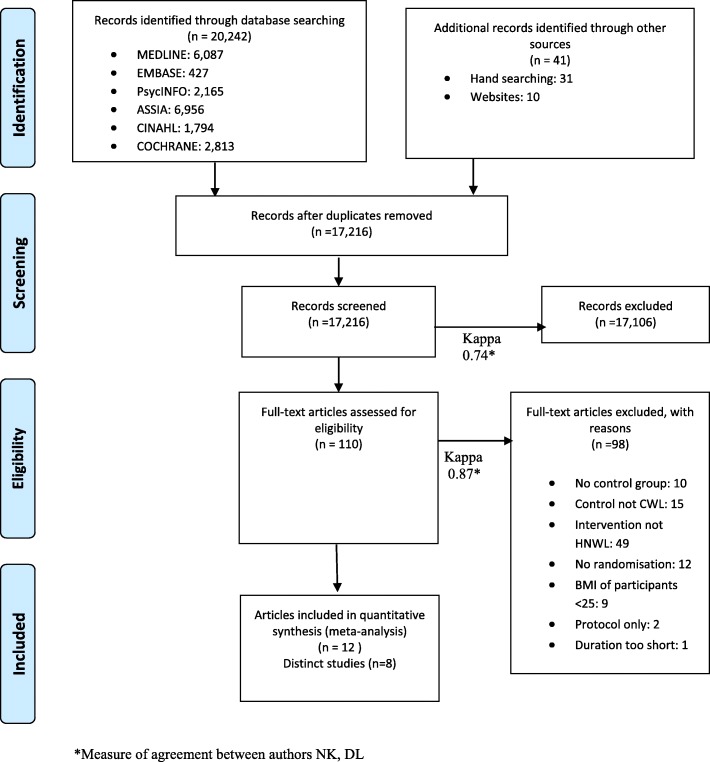
Methods: We searched CENTRAL, MEDLINE, EMBASE, PsycINFO, CINAHL, ASSIA, clinical trial registers, commercial websites and reference lists for randomised controlled trials comparing the two programmes (initially searched up to August 2015 and searched updated to 5 April 2019). We used the Mantel-Haneszel fixed-effect model to pool results. Sub-group and sensitivity analyses that accounted for variations in length of follow-up, enhanced programmes and risk of bias dealt with heterogeneity.
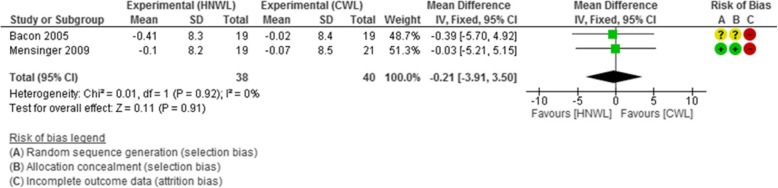
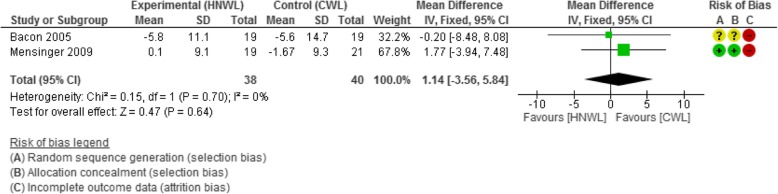
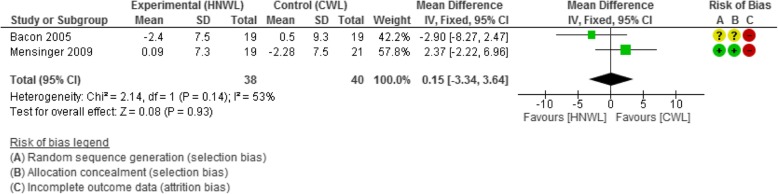
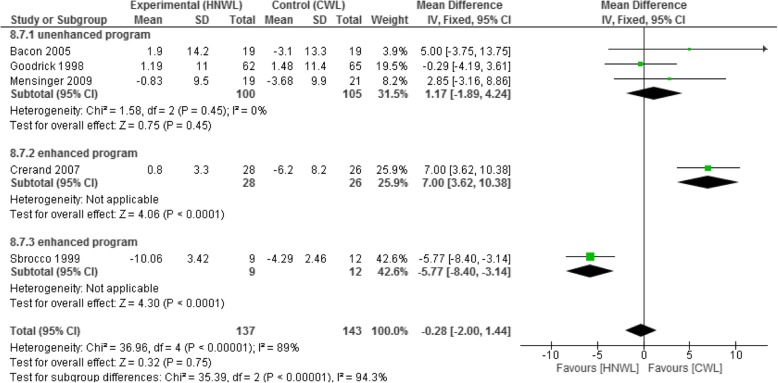
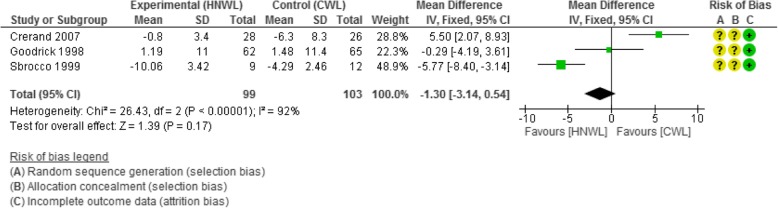
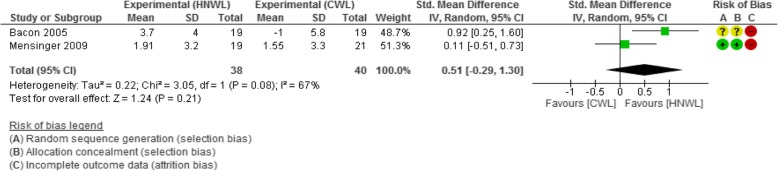
Results: Eight randomised controlled trials of 20,242 potential studies were included. Improvements in total cholesterol-HDL ratio (mean difference - 0.21 mmol/L, 95% confidence interval [- 3.91, 3.50]) and weight loss (- 0.28 kg [- 2.00, 1.44]) favoured HNWL compared to CWL programmes in the long term (53-104 week follow-up), whereas improvements in systolic (- 1.14 mmHg, [- 5.84, 3.56]) and diastolic (- 0.15 mmHg, [- 3.64, 3.34]) blood pressure favoured CWL programmes. These differences did not reach statistical significance. Statistically significant improvements in body satisfaction (- 4.30 [- 8.32, - 0.28]) and restrained eating behaviour (- 4.30 [- 6.77, - 1.83]) favoured HNWL over CWL programmes.
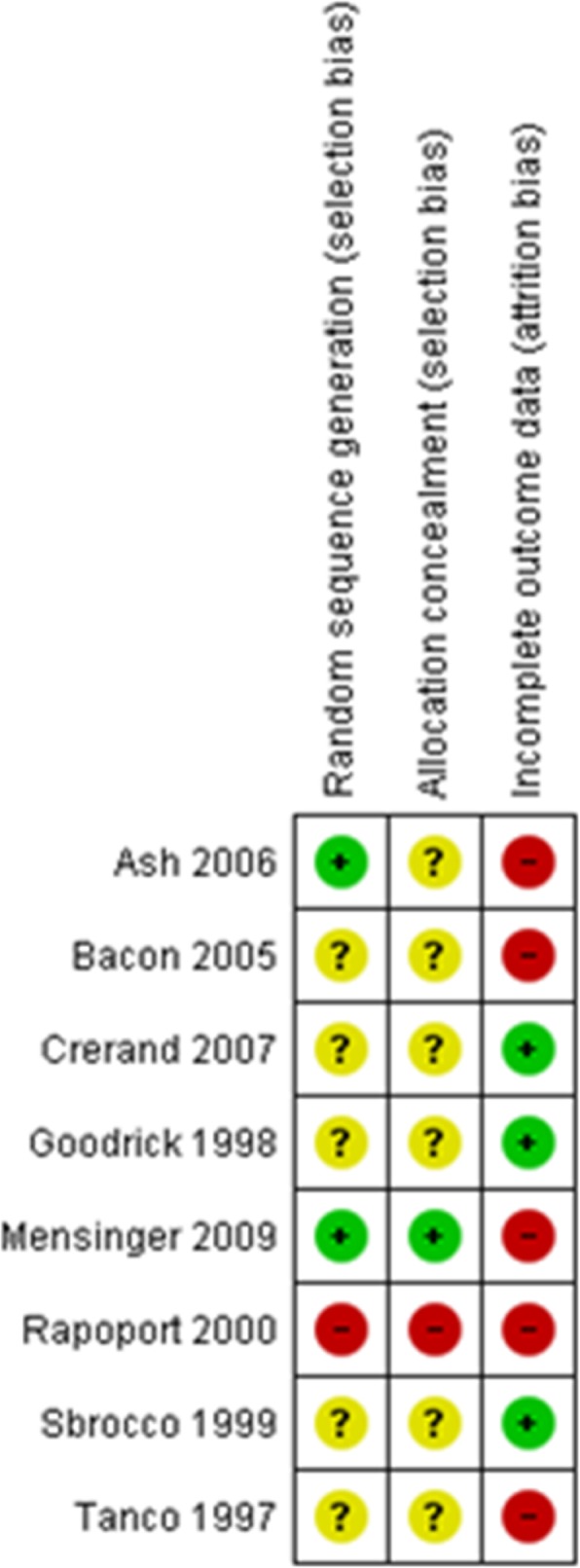
Conclusions: We found no long-term significant differences in improved CVD risk factors; however, body satisfaction and restrained eating behaviour improved more with HNWL compared to CWL programmes. Yet firm conclusions cannot be drawn from small studies with high losses to follow-up and data sometimes arising from a single small study.
Systematic review registration: PROSPERO CRD42015019505.
Keywords: Cardiovascular disease; Disordered eating behaviour; Intuitive eating; Meta-analysis; Non-diet; Obesity; Systematic review; Weight loss; Well-being.
Conflict of interest statement
DL has received vouchers from Slimming World for conducting a previous trial. NK has found the HNWL approach personally helpful to her health. The other authors declare that they have no competing interests.
Figures
References
-
- World Health Organization. Obesity and overweight. www.who.int/mediacentre/factsheets/fs311/en/index.html. Accessed 17 Oct 2013.
-
- Yusuf S, Hawken S, Ôunpuu S, Dans T, Avezum A, Lanas F, McQueen M, Budaj A, Pais P, Varigos J, Lisheng L. Effect of potentially modifiable risk factors associated with myocardial infarction in 52 countries (the INTERHEART study): case-control study. Lancet. 2004;364(9438):937–952. - PubMed
-
- Graham I, Atar D, Borch-Johnsen K, Boysen G, Burell G, Cifkova R, et al. European guidelines on cardiovascular disease prevention in clinical practice: executive summary. Fourth Joint Task Force of the European Society of Cardiology and other societies on cardiovascular disease prevention in clinical practice (constituted by representatives of nine societies and by invited experts) Eur J Cardiovasc Prev Rehabil. 2007;14(Suppl 2):E1–40. - PubMed
-
- Estruch R, Ros E, Salas-Salvadó J, Covas MI, Corella D, Arós F, et al. Primary prevention of cardiovascular disease with a mediterranean diet. N Eng J Med. 2013;368(14):1279–1290. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
