

The Adiponectin-AdipoR1 Axis Mediates Tumor Progression and Tyrosine Kinase Inhibitor Resistance in Metastatic Renal Cell Carcinoma
- PMID: 31401413
- PMCID: PMC6700451
- DOI: 10.1016/j.neo.2019.07.004
The Adiponectin-AdipoR1 Axis Mediates Tumor Progression and Tyrosine Kinase Inhibitor Resistance in Metastatic Renal Cell Carcinoma
Abstract
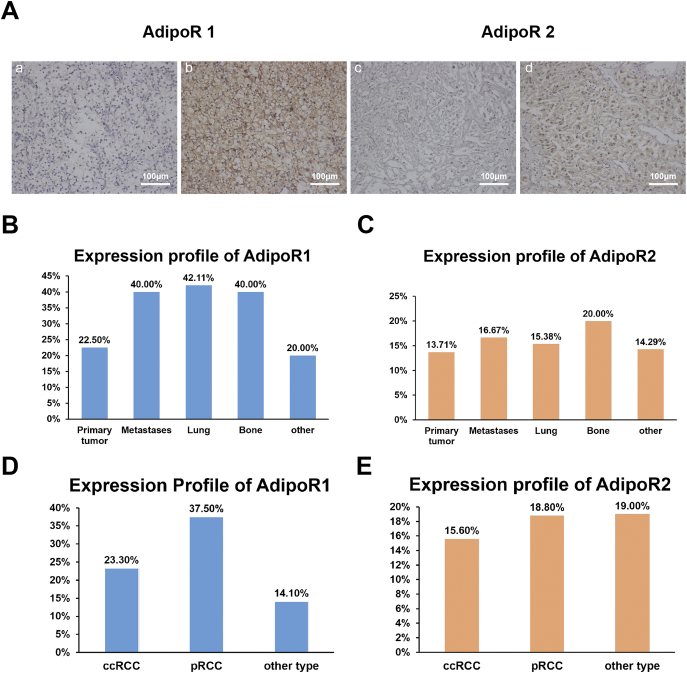
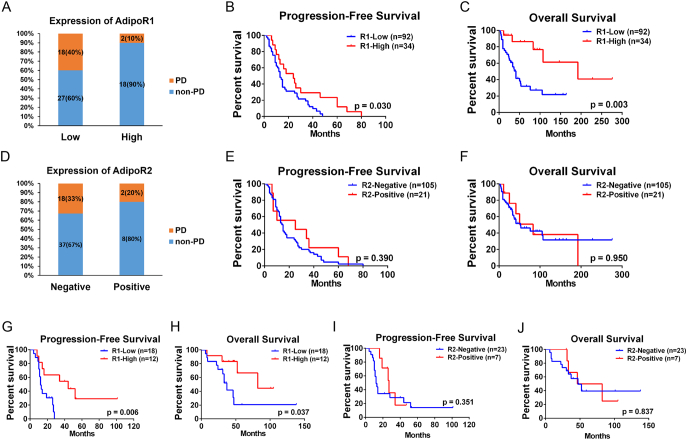
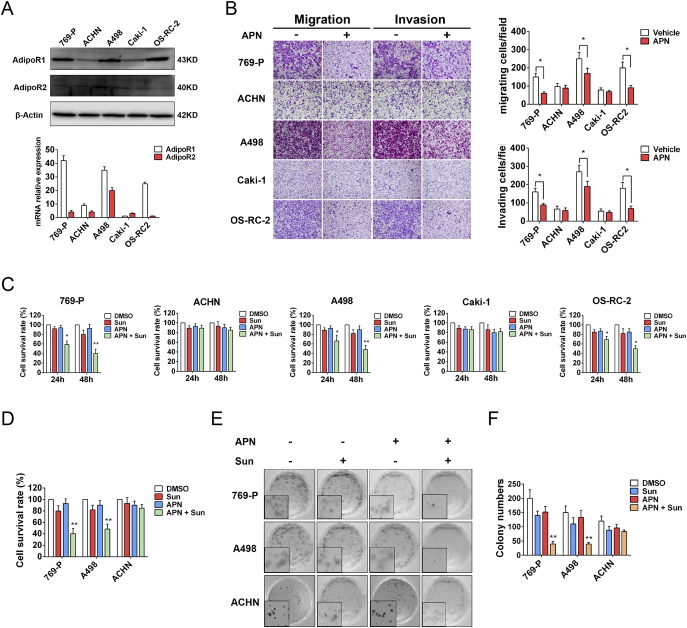
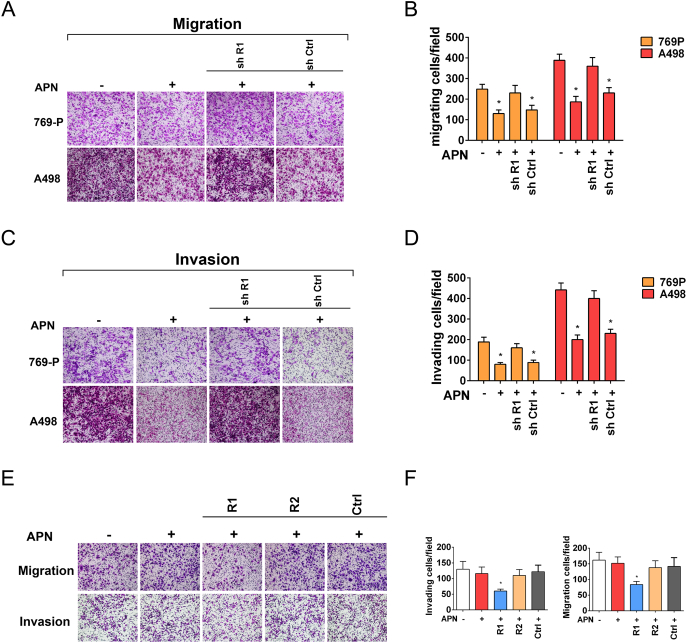
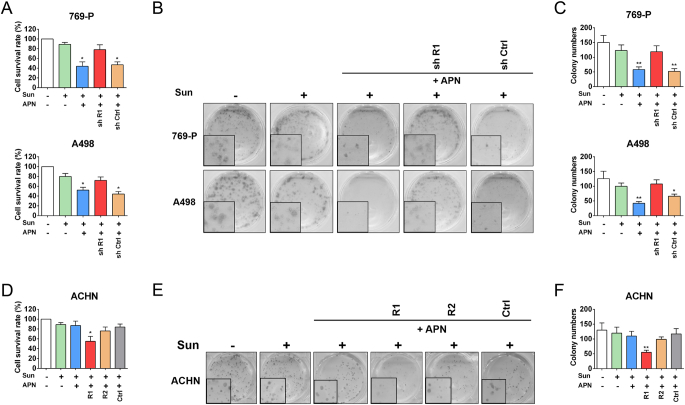
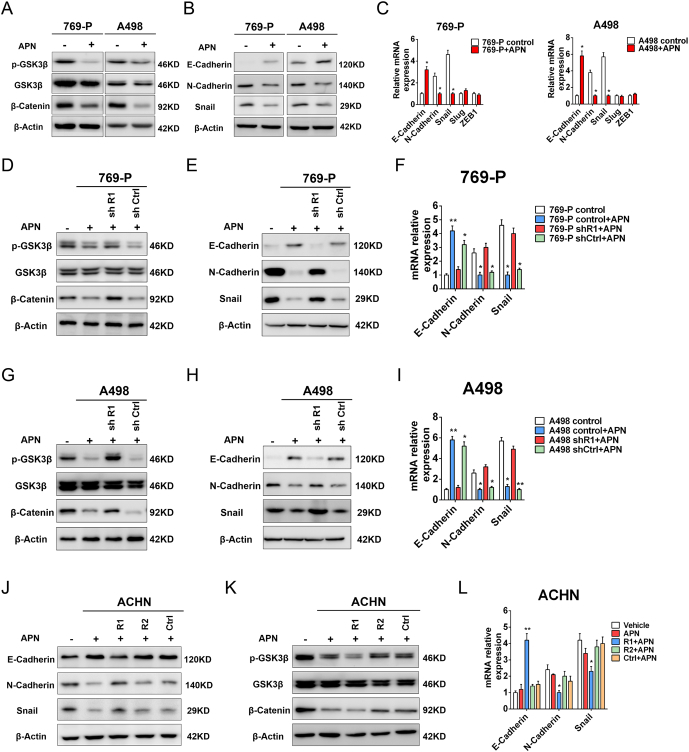
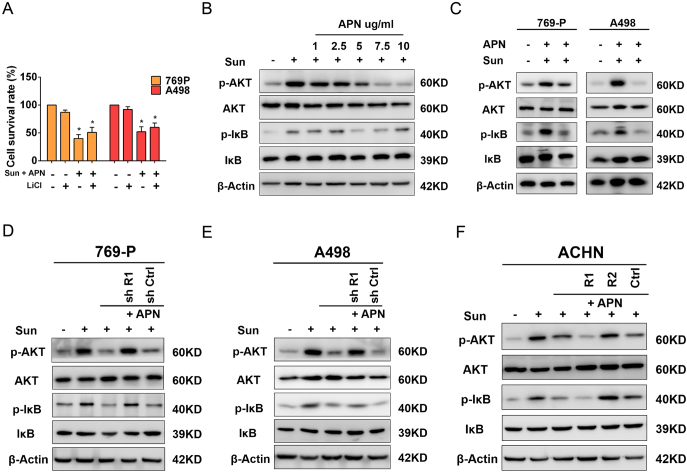
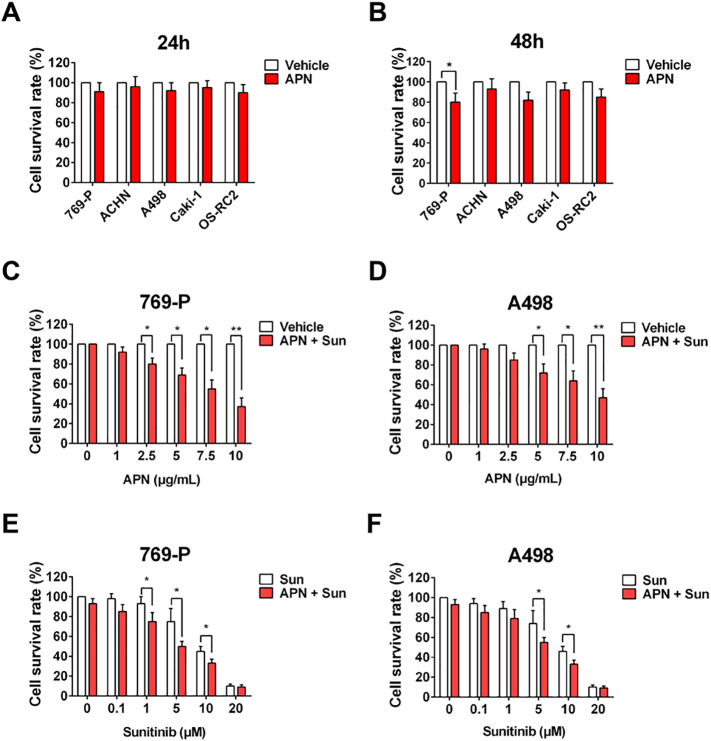
The survival of patients diagnosed with metastatic renal cell carcinoma (RCC) is still limited and the current targeted therapies are only partially effective. Herein, we investigated the clinical value and functions of adiponectin receptors (AdipoR1 and AdipoR2) in metastatic renal cell carcinoma (RCC) patients treated with tyrosine kinase inhibitors (TKIs). A total of 127 mRCC patients treated with first-line TKIs between 2008 and 2017 at a single institution were collected. AdipoR1 and AdipoR2 expression was assessed by immunohistochemistry. AdipoR1 was positively expressed in 87.4% (111/127) of tumors, especially, highly expressed in pulmonary and bone lesions. Patients with low-AdipoR1 expression in primary tumor tissues were more likely to suffer from progressive disease during TKIs treatment (40.0% vs. 11.1%, P = 0 .02), and with decreased progression-free survival (PFS: 19.5 vs. 37.8 mo, P = .001) and overall survival (OS: 62.3 vs 101.1 mo, P = .004) compared to those with high-AdipoR1 expression. Moreover, low-AdipoR1 expression in metastatic tissues was also associated with poor PFS (P = .006) and OS (P = .037). In contrast, AdipoR2 expression was neither associated with sunitinib response nor patient survival. In vitro, we found that adiponectin inhibited migration, invasion and sensitized RCC cells to sunitinib though interacting with AdipoR1, but not AdipoR2. Furthermore, we demonstrated that adiponentin-AdipoR1 axis inhibits tumor cells migration and invasion by blocking the GSK3β/β-Catenin pathway and enhances sunitinib sensitivity via abrogating PI3K/AKT/NF-κB signaling. Our results suggest that adiponentin-AdipoR1 axis may serve as a predictor of TKIs response and could be a potential therapeutic target in the future treatment for metastatic RCC.
Copyright © 2019 The Authors. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Siegel RL, Miller KD. Jemal A (2018). Cancer statistics. CA Cancer J Clin. 2018;68:7–30. - PubMed
-
- Sun M, Shariat SF, Cheng C, Ficarra V, Murai M, Oudard S, Pantuck AJ, Zigeuner R, Karakiewicz PI. Prognostic factors and predictive models in renal cell carcinoma: a contemporary review. Eur Urol. 2011;60:644–661. - PubMed
-
- Rini BI, Atkins MB. Resistance to targeted therapy in renal-cell carcinoma. Lancet Oncol. 2009;10:992–1000. - PubMed
-
- Molina A, Lin X, Korytowsky B, Matczak E, Lechuga M, Wiltshire R, Motzer R. Sunitinib objective response in metastatic renal cell carcinoma: analysis of 1059 patients treated on clinical trials. Eur J Cancer. 2014;50:351–358. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
