

Changes in Plant-Based Diet Quality and Total and Cause-Specific Mortality
- PMID: 31401846
- PMCID: PMC6746589
- DOI: 10.1161/CIRCULATIONAHA.119.041014
Changes in Plant-Based Diet Quality and Total and Cause-Specific Mortality
Abstract
Background: Plant-based diets have been associated with lower risk of type 2 diabetes mellitus and cardiovascular disease (CVD) and are recommended for both health and environmental benefits. However, the association between changes in plant-based diet quality and mortality remains unclear.
Methods: We investigated the associations between 12-year changes (from 1986 to 1998) in plant-based diet quality assessed by 3 plant-based diet indices (score range, 18-90)-an overall plant-based diet index (PDI), a healthful PDI, and an unhealthful PDI-and subsequent total and cause-specific mortality (1998-2014). Participants were 49 407 women in the Nurses' Health Study (NHS) and 25 907 men in the Health Professionals Follow-Up Study (HPFS) who were free from CVD and cancer in 1998. Multivariable-adjusted Cox proportional-hazards models were used to estimate hazard ratios (HRs) and 95% CIs.
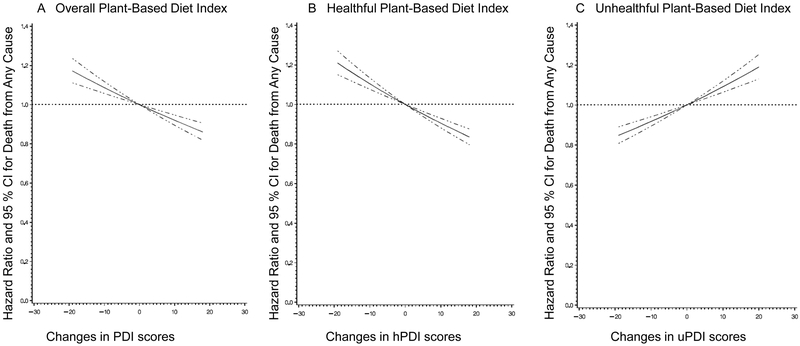
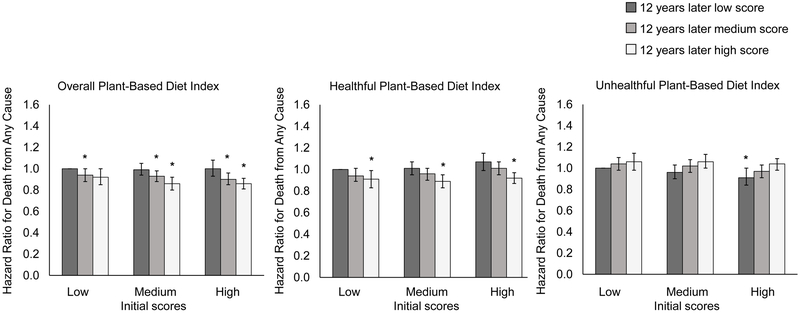
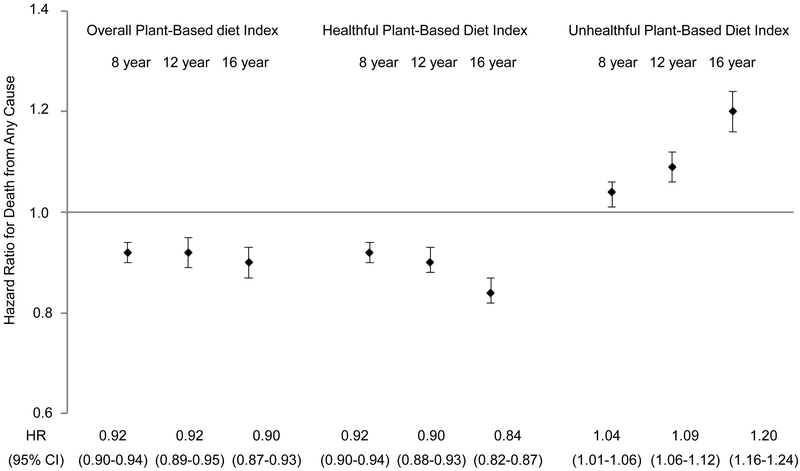
Results: We documented 10 686 deaths including 2046 CVD deaths and 3091 cancer deaths in the NHS over 725 316 person-years of follow-up and 6490 deaths including 1872 CVD deaths and 1772 cancer deaths in the HPFS over 371 322 person-years of follow-up. Compared with participants whose indices remained stable, among those with the greatest increases in diet scores (highest quintile), the pooled multivariable-adjusted HRs for total mortality were 0.95 (95% CI, 0.90-1.00) for PDI, 0.90 (95% CI, 0.85-0.95) for healthful PDI, and 1.12 (95% CI, 1.07-1.18) for unhealthful PDI. Among participants with the greatest decrease (lowest quintile), the multivariable-adjusted HRs were 1.09 (95% CI, 1.04-1.15) for PDI, 1.10 (95% CI, 1.05-1.15) for healthful PDI, and 0.93 (95% CI, 0.88-0.98) for unhealthful PDI. For CVD mortality, the risk associated with a 10-point increase in each PDI was 7% lower (95% CI, 1-12%) for PDI, 9% lower (95% CI, 4-14%) for healthful PDI, and 8% higher (95% CI, 2-14%) for unhealthful PDI. There were no consistent associations between changes in plant-based diet indices and cancer mortality.
Conclusions: Improving plant-based diet quality over a 12-year period was associated with a lower risk of total and CVD mortality, whereas increased consumption of an unhealthful plant-based diet was associated with a higher risk of total and CVD mortality.
Keywords: death; diet; epidemiology; food quality; vegetarian diet.
Conflict of interest statement
Disclosures
Dr. Li and Dr. Hu reported receiving research support from California Walnut Commission. Dr. Satija is currently employed at Analysis Group, Inc. All other authors have no conflict of interest to disclose.
Figures
References
-
- Millen BE, Abrams S, Adams-Campbell L, Anderson CA, Brenna JT, Campbell WW, Clinton S, Hu F, Nelson M, Neuhouser ML, Perez-Escamilla R, Siega-Riz AM, Story M and Lichtenstein AH. The 2015 Dietary Guidelines Advisory Committee Scientific Report: Development and Major Conclusions. Adv Nutr. 2016;7:438–444. doi: 10.3945/an.116.012120 - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
