

Antibiotic prophylaxis in the surgical management of miscarriage in low-income countries: a cost-effectiveness analysis of the AIMS trial
- PMID: 31402008
- PMCID: PMC6695526
- DOI: 10.1016/S2214-109X(19)30336-5
Antibiotic prophylaxis in the surgical management of miscarriage in low-income countries: a cost-effectiveness analysis of the AIMS trial
Abstract
Background: There is ongoing debate on the clinical benefits of antibiotic prophylaxis for reducing pelvic infection after miscarriage surgery. We aimed to study the cost-effectiveness of antibiotic prophylaxis in the surgical management of miscarriage in low-income countries.
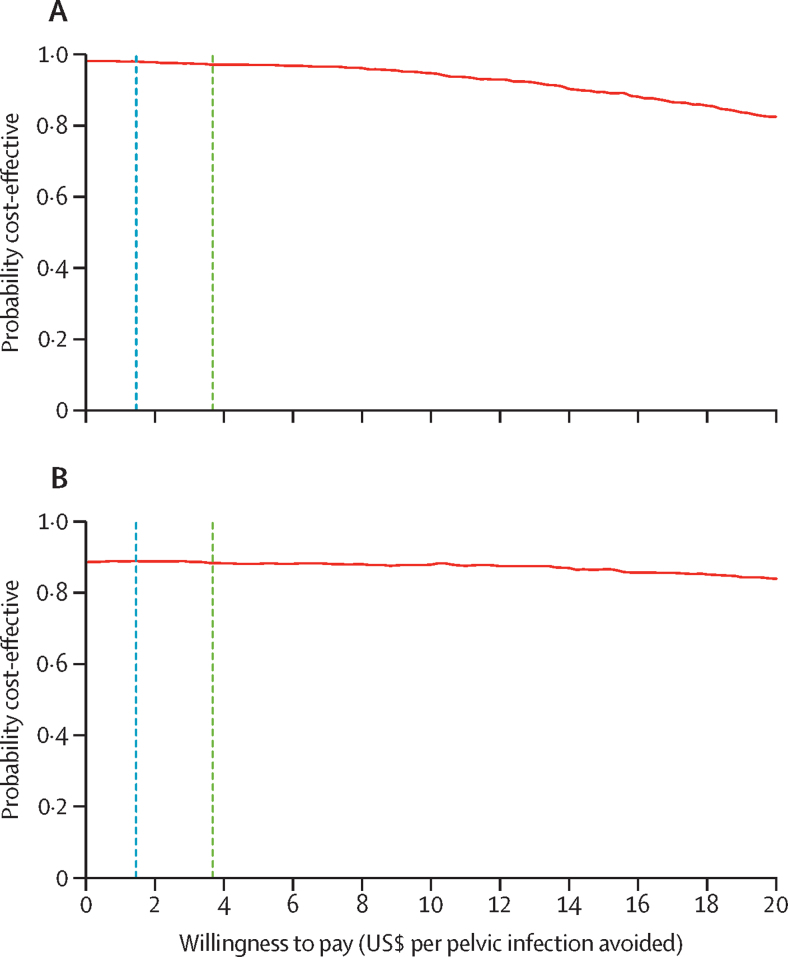
Methods: We did an incremental cost-effectiveness analysis using data from 3412 women recruited to the AIMS trial, a randomised, double-blind, placebo-controlled trial designed to evaluate the effectiveness of antibiotic prophylaxis in the surgical management of miscarriage in Malawi, Pakistan, Tanzania, and Uganda. Economic evaluation was done from a health-care-provider perspective on the basis of the outcome of cost per pelvic infection avoided within 2 weeks of surgery. Pelvic infection was broadly defined by the presence of clinical features or the clinically identified need to administer antibiotics. We used non-parametric bootstrapping and multilevel random effects models to estimate incremental mean costs and outcomes. Decision uncertainty was shown via cost-effectiveness acceptability frontiers. The AIMS trial is registered with the ISRCTN registry, number ISRCTN97143849.
Findings: Between June 2, 2014, and April 26, 2017, 3412 women were assigned to receive either antibiotic prophylaxis (1705 [50%] of 3412) or placebo (1707 [50%] of 3412) in the AIMS trial. 158 (5%) of 3412 women developed pelvic infection within 2 weeks of surgery, of whom 68 (43%) were in the antibiotic prophylaxis group and 90 (57%) in the placebo group. There is 97-98% probability that antibiotic prophylaxis is a cost-effective intervention at expected thresholds of willingness-to-pay per additional pelvic infection avoided. In terms of post-surgery antibiotics, the antibiotic prophylaxis group was US$0·27 (95% CI -0·49 to -0·05) less expensive per woman than the placebo group. A secondary analysis, a sensitivity analysis, and all subgroup analyses supported these findings. Antibiotic prophylaxis, if implemented routinely before miscarriage surgery, could translate to an annual total cost saving of up to $1·4 million across the four participating countries and up to $8·5 million across the two regions of sub-Saharan Africa and south Asia.
Interpretation: Antibiotic prophylaxis is more effective and less expensive than no antibiotic prophylaxis. Policy makers in various settings should be confident that antibiotic prophylaxis in miscarriage surgery is cost-effective.
Funding: UK Medical Research Council, Wellcome Trust, and the UK Department for International Development.
Copyright © 2019 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Figures
Comment in
-
It is cost effective to improve the standard of care for women experiencing miscarriage.Lancet Glob Health. 2019 Sep;7(9):e1164-e1165. doi: 10.1016/S2214-109X(19)30314-6. Lancet Glob Health. 2019. PMID: 31401994 Free PMC article. No abstract available.
References
-
- Sedgh G, Singh S, Shah IH, Åhman E, Henshaw SK, Bankole A. Induced abortion: incidence and trends worldwide from 1995 to 2008. Lancet. 2012;379:625–632. - PubMed
-
- Wilcox AJ, Weinberg CR, O'Connor JF. Incidence of early loss of pregnancy. N Engl J Med. 1988;319:189–194. - PubMed
-
- WHO . World Health Organization; Geneva: 2014. Clinical practice handbook for safe abortion. - PubMed
-
- RCOG . Royal College of Obstetricians and Gynaecologists; London, UK: 2015. Best practice in comprehensive abortion care (Best Practice Paper No 2)
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
