

Airway hypoxia in lung transplantation
- PMID: 31403087
- PMCID: PMC6688850
- DOI: 10.1016/j.cophys.2018.12.002
Airway hypoxia in lung transplantation
Abstract
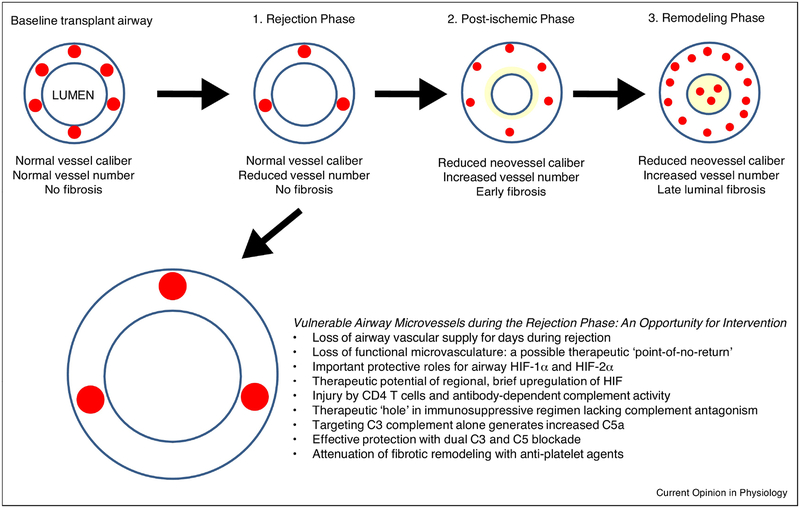
Lung transplantation is a life-saving operation for patients with advanced lung disease. Pulmonary allografts eventually fail because of infection, thromboembolism, malignancy, airway complications, and chronic rejection, otherwise known as chronic lung allograft dysfunction (CLAD). Emerging evidence suggests that a highly-compromised airway circulation contributes to the evolution of airway complications and CLAD. There are two significant causes of poor perfusion and airway hypoxia in lung transplantation: an abnormal bronchial circulation which causes airway complications and microvascular rejection which induces CLAD. At the time of transplantation, the bronchial artery circulation, a natural component of the airway circulatory anatomy, is not surgically connected, and bronchi distal to the anastomosis become hypoxic. Subsequently, the bronchial anastomosis is left to heal under ischemic conditions. Still later, the extant microvessels in transplant bronchi are subjected to alloimmune insults that can further negatively impact pulmonary function. This review describes how airway tissue hypoxia evolves in lung transplantation, why depriving oxygenation in the bronchi and more distal bronchioles contributes to disease pathology and what therapeutic interventions are currently emerging to address these vascular injuries. Improving anastomotic vascular healing at the time of transplantation and preventing microvascular loss during acute rejection episodes are two steps that could limit airway hypoxia and improve patient outcomes.
Keywords: anastomosis; hypoxia; hypoxia-inducible factors; lung transplantation; microvasculature.
Conflict of interest statement
Declaration of Interest: Mark Nicolls, is an inventor on a patent that is directly germane to the ideas that are proposed in this review. U.S. Application Serial No. 14/653,245 Entitled: Iron Chelators and Use Thereof for Reducing Transplant Failure During Rejection Episodes First Named Inventor: Nicolls, Mark R. Your Ref.: S11–300; C11657_P11657–03 Our Ref.: STAN-891 Patent No. 9763899. Although, only in its incipient stages, a company, which Mark Nicolls is involved with, is being formed around the concept of using iron chelators in lung transplant recipients, which is a concept referred to multiple times as a promising approach within the manuscript.
Figures

Similar articles
-
Bronchial anastomotic complications as a microvascular disruption in a mouse model of airway transplantation.Front Immunol. 2025 May 14;16:1567657. doi: 10.3389/fimmu.2025.1567657. eCollection 2025. Front Immunol. 2025. PMID: 40438113 Free PMC article. Review.
-
Lung transplant airway hypoxia: a diathesis to fibrosis?Am J Respir Crit Care Med. 2010 Jul 15;182(2):230-6. doi: 10.1164/rccm.200910-1573OC. Epub 2010 Mar 25. Am J Respir Crit Care Med. 2010. PMID: 20339145 Free PMC article.
-
Hypoxic Gene Expression of Donor Bronchi Linked to Airway Complications after Lung Transplantation.Am J Respir Crit Care Med. 2016 Mar 1;193(5):552-60. doi: 10.1164/rccm.201508-1634OC. Am J Respir Crit Care Med. 2016. PMID: 26488115 Free PMC article.
-
Promotion of airway anastomotic microvascular regeneration and alleviation of airway ischemia by deferoxamine nanoparticles.Biomaterials. 2014 Jan;35(2):803-813. doi: 10.1016/j.biomaterials.2013.09.092. Epub 2013 Oct 22. Biomaterials. 2014. PMID: 24161166 Free PMC article.
-
The Bronchial Arterial Circulation in Lung Transplantation: Bedside to Bench to Bedside, and Beyond.Transplantation. 2018 Aug;102(8):1240-1249. doi: 10.1097/TP.0000000000002180. Transplantation. 2018. PMID: 29557912 Review.
Cited by
-
Preservation of bronchial artery circulation on ex-vivo lung perfusion.Sci Rep. 2025 Jul 2;15(1):23354. doi: 10.1038/s41598-025-06174-8. Sci Rep. 2025. PMID: 40603432 Free PMC article.
-
Auto-inflammation and auto-immunity pathways are associated with emergence of BOS in pediatric lung transplantation.Pediatr Transplant. 2022 Jun;26(4):e14247. doi: 10.1111/petr.14247. Epub 2022 Feb 10. Pediatr Transplant. 2022. PMID: 35146849 Free PMC article.
-
Analysis of nosocomial infection and risk factors in lung transplant patients: a case-control study.Ann Transl Med. 2022 Jul;10(14):804. doi: 10.21037/atm-22-3023. Ann Transl Med. 2022. PMID: 35965837 Free PMC article.
-
Emerging trends and hotspots in animal experimental research on lung transplantation from 2004 to 2023: a bibliometric analysis.J Thorac Dis. 2025 Feb 28;17(2):796-815. doi: 10.21037/jtd-24-1451. Epub 2025 Feb 27. J Thorac Dis. 2025. PMID: 40083532 Free PMC article.
-
The complex anatomy of the bronchial arteries: a meta-analysis with potential implications for thoracic surgery and hemoptysis treatment.Sci Rep. 2024 Dec 28;14(1):30942. doi: 10.1038/s41598-024-81935-5. Sci Rep. 2024. PMID: 39730654 Free PMC article.
References
-
- Chambers DC, Yusen RD, Cherikh WS, Goldfarb SB, Kucheryavaya AY, Khusch K, Levvey BJ, Lund LH, Meiser B, Rossano JW, Stehlik J: The registry of the international society for heart and lung transplantation: Thirty-fourth adult lung and heart-lung transplantation report-2017; focus theme: Allograft ischemic time. The Journal of heart and lung transplantation : the official publication of the International Society for Heart Transplantation (2017) 36(10):1047–1059. - PubMed
-
-
Crespo MM, McCarthy DP, Hopkins PM, Clark SC, Budev M, Bermudez CA, Benden C, Eghtesady P, Lease ED, Leard L, D’Cunha J et al.: Ishlt consensus statement on adult and pediatric airway complications after lung transplantation: Definitions, grading system, and therapeutics. The Journal of heart and lung transplantation : the official publication of the International Society for Heart Transplantation (2018) 37(5):548–563.
* The problem of airway complications following transplantation is described and a pathological grading scale is proposed which may help guide future clinical trials which seek to prevent and treat this important lung transplant morbidity.
-
-
- Luckraz H, Goddard M, McNeil K, Atkinson C, Charman SC, Stewart S, Wallwork J: Microvascular changes in small airways predispose to obliterative bronchiolitis after lung transplantation. The Journal of heart and lung transplantation : the official publication of the International Society for Heart Transplantation (2004) 23(5):527–531. - PubMed
-
- Luckraz H, Goddard M, McNeil K, Atkinson C, Sharples LD, Wallwork J: Is obliterative bronchiolitis in lung transplantation associated with microvascular damage to small airways? Ann Thorac Surg (2006) 82(4):1212–1218. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources