

Evaluation of the Cascade of Diabetes Care in the United States, 2005-2016
- PMID: 31403657
- PMCID: PMC6692836
- DOI: 10.1001/jamainternmed.2019.2396
Evaluation of the Cascade of Diabetes Care in the United States, 2005-2016
Abstract
Importance: Treatment advances in diabetes can meaningfully improve outcomes only if they effectively reach the populations at risk.
Objectives: To evaluate whether the cascade of US diabetes care, defined as diabetes diagnosis, linkage to care, and achievement of individual and combined treatment targets, improved from 2005 to 2016 and to investigate potential disparities in US diabetes care.
Design, setting, and participants: Nationally representative, serial cross-sectional studies included in the 2005-2016 National Health and Nutrition Examination Survey were evaluated. Data on nonpregnant US adults (age ≥18 years) with diabetes who had reported fasting for 9 or more hours (n = 1742 diagnosed and 746 undiagnosed) were included. Data analysis was performed from August 1, 2018, to May 10, 2019.
Exposures: Time period (2005-2008, 2009-2012, and 2013-2016), age, sex, race/ethnicity, health insurance, and educational level incorporated into logistic regression models predicting odds of target achievement.
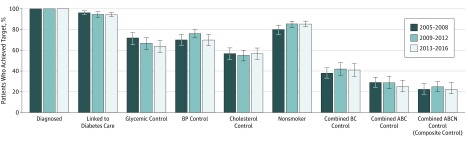
Main outcomes and measures: Proportion of participants overall and stratified by age, sex, and race/ethnicity who were linked to diabetes care and met glycemic (hemoglobin A1c <7.0%-8.5%, depending on age and complications), blood pressure (<140/90 mm Hg), cholesterol level (low-density lipoprotein cholesterol <100 mg/dL), and smoking abstinence targets and a composite of all targets.
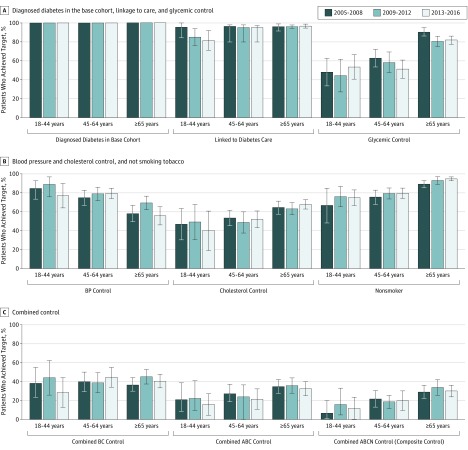
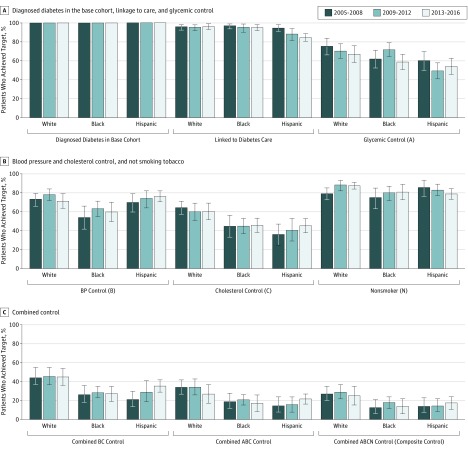
Results: In 2013-2016, of 1742 US adults with diagnosed diabetes, 94% (95% CI, 92%-96%) were linked to diabetes care; 64% (95% CI, 58%-69%) met hemoglobin A1c level, 70% (95% CI, 64%-75%) met blood pressure level, and 57% (95% CI, 51%-62%) met cholesterol level targets; 85% were nonsmokers (95% CI, 82%-88%); and 23% (95% CI, 17%-29%) achieved the composite goal. Results were similar in 2005-2008 (composite 23%) and in 2009-2012 (composite 25%). There was no significant improvement in diagnosis or target achievement during the study period. Compared with middle-aged adults (45-64 years) with diagnosed diabetes, older patients (≥65 years) had higher odds (adjusted odds ratio [aOR], 1.70; 95% CI, 1.17-2.48) and younger adults (18-44 years) had lower odds (aOR, 0.53; 95% CI, 0.29-0.97) of meeting the composite target. Women had lower odds of achieving the composite target than men (aOR, 0.60; 95% CI, 0.45-0.80). Non-Hispanic black individuals vs non-Hispanic white individuals had lower odds of achieving the composite target (aOR, 0.57; 95% CI, 0.39-0.83). Having health insurance was the strongest predictor of linkage to diabetes care (aOR, 3.96; 95% CI, 2.34-6.69).
Conclusions and relevance: It appears that the diabetes care cascade in the United States has not significantly improved between 2005 and 2016. This study's findings suggest that gaps in diabetes care that were present in 2005, particularly among younger adults (18-44 years), women, and nonwhite individuals, persist.
Conflict of interest statement
Figures
Comment in
-
Barriers and Solutions to a Recently Noted Failure of Diabetes Care Outcomes to Improve From 2005 to 2016 in the United States.J Diabetes Sci Technol. 2020 Jan;14(1):189-190. doi: 10.1177/1932296819880861. Epub 2019 Oct 9. J Diabetes Sci Technol. 2020. PMID: 31595785 Free PMC article. No abstract available.
References
-
- Centers for Disease Control and Prevention National diabetes statistics report, 2017. http://www.cdc.gov/diabetes/pdfs/data/statistics/national-diabetes-stati.... Accessed January 28, 2019.
-
- American Diabetes Association Standards of medical care in diabetes—2018. January 2018; https://diabetesed.net/wp-content/uploads/2017/12/2018-ADA-Standards-of-.... Accessed January 28, 2019.
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
