

Axitinib in Combination With Toripalimab, a Humanized Immunoglobulin G4 Monoclonal Antibody Against Programmed Cell Death-1, in Patients With Metastatic Mucosal Melanoma: An Open-Label Phase IB Trial
- PMID: 31403867
- PMCID: PMC6839911
- DOI: 10.1200/JCO.19.00210
Axitinib in Combination With Toripalimab, a Humanized Immunoglobulin G4 Monoclonal Antibody Against Programmed Cell Death-1, in Patients With Metastatic Mucosal Melanoma: An Open-Label Phase IB Trial
Abstract
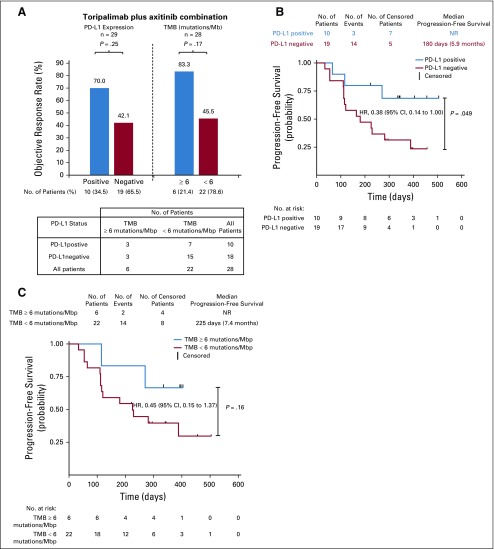
Purpose: Metastatic mucosal melanoma responds poorly to anti-programmed cell death-1 (PD-1) monotherapy. Vascular endothelial growth factor (VEGF) has been shown to play an important immunosuppressive role in the tumor microenvironment. The combination of VEGF inhibition and PD-1 blockade provides therapeutic opportunities for patients refractory to either therapy alone.
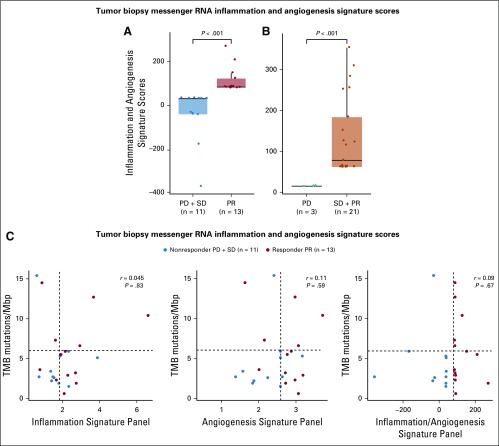
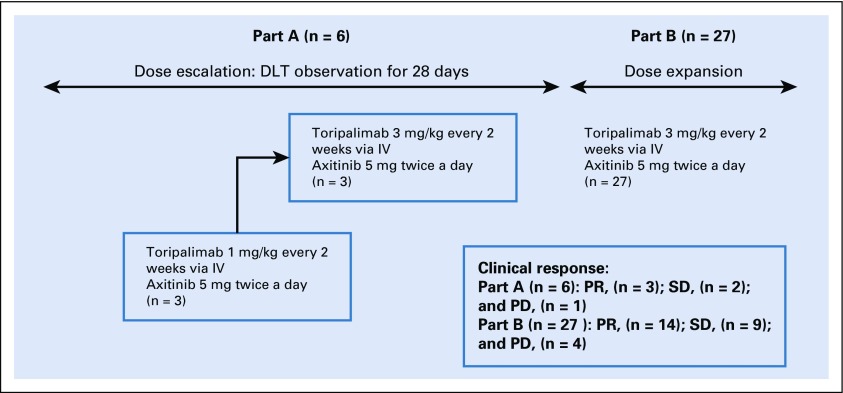
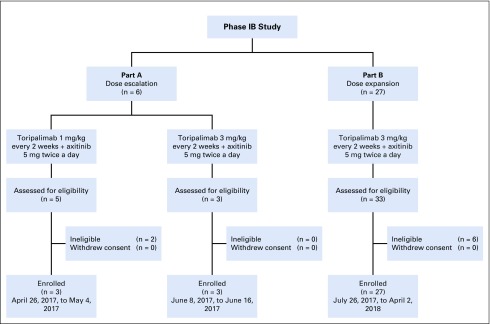
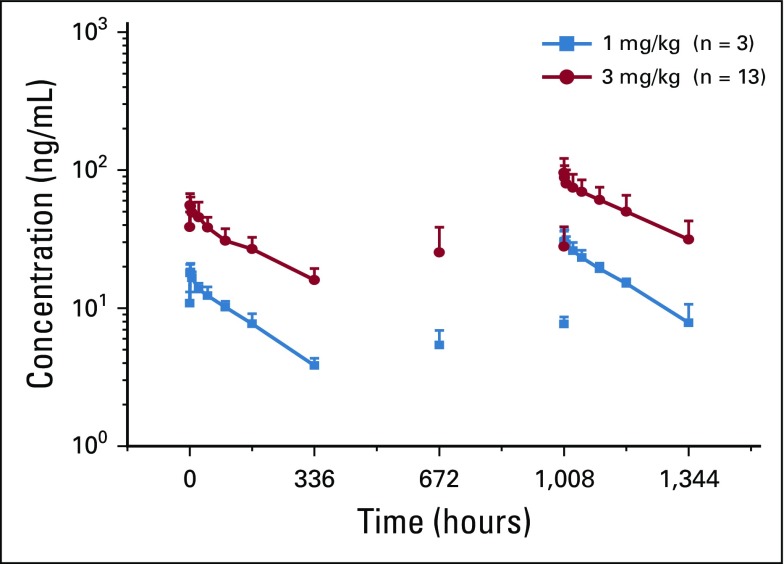
Patients and methods: We conducted a single-center, phase IB trial evaluating the safety and preliminary efficacy of toripalimab, a humanized immunoglobulin G4 monoclonal antibody against PD-1 in combination with the VEGF receptor inhibitor axitinib in patients with advanced melanoma, including patients with chemotherapy-naïve mucosal melanomas (88%). Patients received toripalimab at 1 or 3 mg/kg via intravenous infusion every 2 weeks, in combination with axitinib 5 mg orally twice a day, in a dose-escalation and cohort-expansion study until confirmed disease progression, unacceptable toxicity, or voluntary withdrawal. The primary objective was safety. Secondary objectives included efficacy, pharmacokinetics, pharmacodynamics, immunogenicity, and tumor tissue biomarkers.
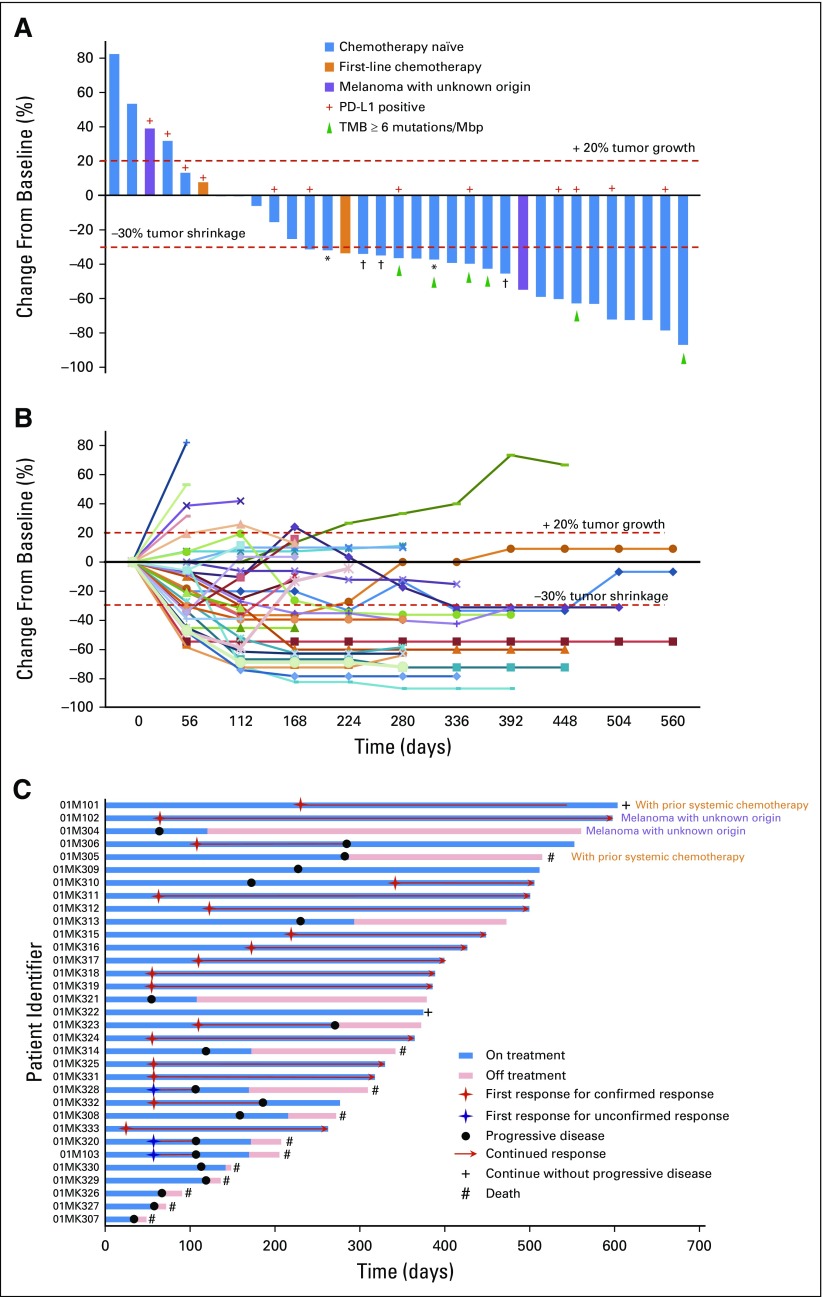
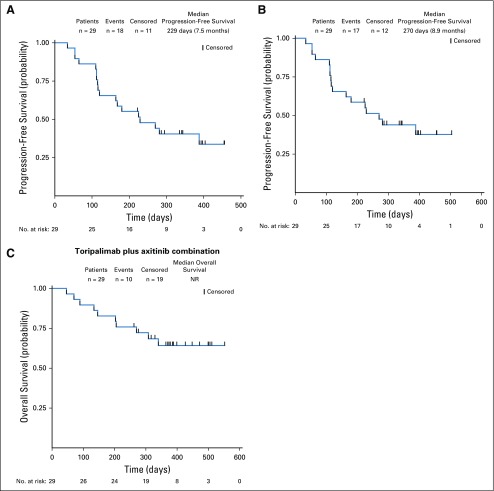
Results: Thirty-three patients were enrolled. No dose-limiting toxicities were observed. Ninety-seven percent of patients experienced treatment-related adverse events (TRAEs). The most common TRAEs were mild (grade 1 or 2) and included diarrhea, proteinuria, hand and foot syndrome, fatigue, AST or ALT elevation, hypertension, hypo- or hyperthyroidism, and rash. Grade 3 or greater TRAEs occurred in 39.4% of patients. By the cutoff date, among 29 patients with chemotherapy-naïve mucosal melanoma, 14 patients (48.3%; 95% CI, 29.4% to 67.5%) achieved objective response, and the median progression-free survival time was 7.5 months (95% CI, 3.7 months to not reached) per Response Evaluation Criteria in Solid Tumors (RECIST) version 1.1.
Conclusion: The combination of toripalimab plus axitinib was tolerable and showed promising antitumor activity in patients with treatment-naïve metastatic mucosal melanoma. Patients enrolled in this study were all Asian, and this combination therapy must be validated in a randomized phase III trial that includes a non-Asian population before it can become a standard of care.
Figures
References
-
- Chang AE, Karnell LH, Menck HR. The National Cancer Data Base report on cutaneous and noncutaneous melanoma: A summary of 84,836 cases from the past decade—The American College of Surgeons Commission on Cancer and the American Cancer Society. Cancer. 1998;83:1664–1678. - PubMed
-
- Chan KK, Chan RC, Ho RS, et al. Clinical patterns of melanoma in Asians: 11-year experience in a tertiary referral center. Ann Plast Surg. 2016;77(suppl 1):S6–S11. - PubMed
-
- Hayward NK, Wilmott JS, Waddell N, et al. Whole-genome landscapes of major melanoma subtypes. Nature. 2017;545:175–180. - PubMed
-
- Wang X, Si L, Guo J. Treatment algorithm of metastatic mucosal melanoma. Linchuang Zhongliuxue Zazhi. 2014;3:38. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
