

Intraoperative Mechanical Ventilation and Postoperative Pulmonary Complications after Cardiac Surgery
- PMID: 31403976
- PMCID: PMC6800803
- DOI: 10.1097/ALN.0000000000002909
Intraoperative Mechanical Ventilation and Postoperative Pulmonary Complications after Cardiac Surgery
Erratum in
-
Intraoperative Mechanical Ventilation and Postoperative Pulmonary Complications after Cardiac Surgery: Erratum.Anesthesiology. 2020 Jan;132(1):217. doi: 10.1097/ALN.0000000000003038. Anesthesiology. 2020. PMID: 31651530 No abstract available.
Abstract
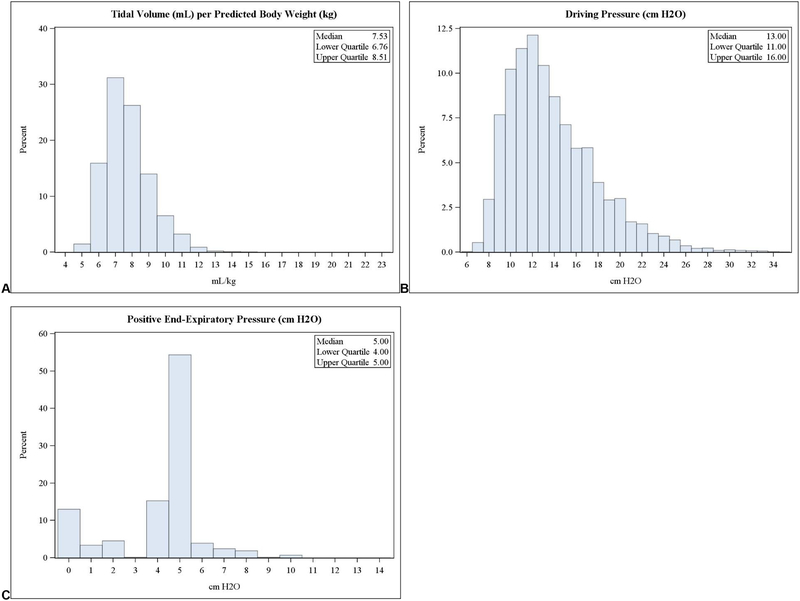
Background: Compared with historic ventilation strategies, modern lung-protective ventilation includes lower tidal volumes (VT), lower driving pressures, and application of positive end-expiratory pressure (PEEP). The contributions of each component to an overall intraoperative protective ventilation strategy aimed at reducing postoperative pulmonary complications have neither been adequately resolved, nor comprehensively evaluated within an adult cardiac surgical population. The authors hypothesized that a bundled intraoperative protective ventilation strategy was independently associated with decreased odds of pulmonary complications after cardiac surgery.
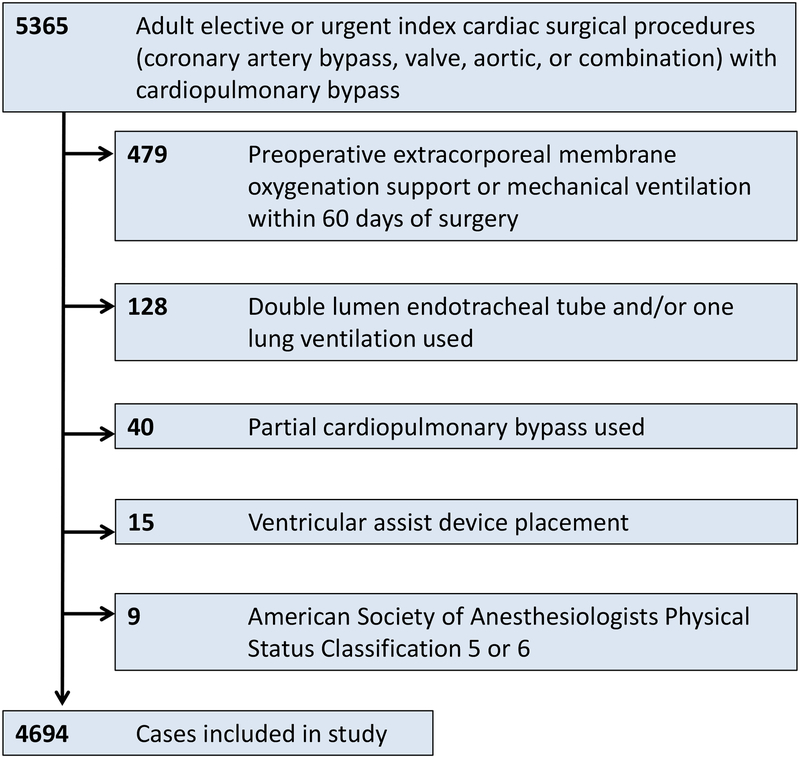
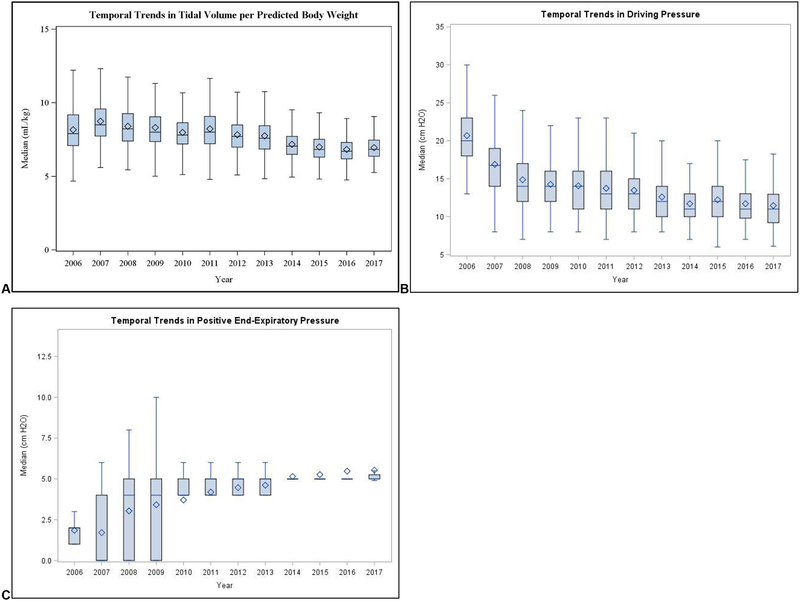
Methods: In this observational cohort study, the authors reviewed nonemergent cardiac surgical procedures using cardiopulmonary bypass at a tertiary care academic medical center from 2006 to 2017. The authors tested associations between bundled or component intraoperative protective ventilation strategies (VT below 8 ml/kg ideal body weight, modified driving pressure [peak inspiratory pressure - PEEP] below 16 cm H2O, and PEEP greater than or equal to 5 cm H2O) and postoperative outcomes, adjusting for previously identified risk factors. The primary outcome was a composite pulmonary complication; secondary outcomes included individual pulmonary complications, postoperative mortality, as well as durations of mechanical ventilation, intensive care unit stay, and hospital stay.
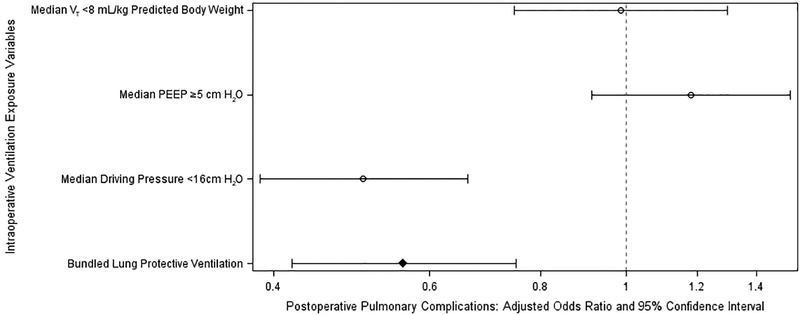
Results: Among 4,694 cases reviewed, 513 (10.9%) experienced pulmonary complications. After adjustment, an intraoperative lung-protective ventilation bundle was associated with decreased pulmonary complications (adjusted odds ratio, 0.56; 95% CI, 0.42-0.75). Via a sensitivity analysis, modified driving pressure below 16 cm H2O was independently associated with decreased pulmonary complications (adjusted odds ratio, 0.51; 95% CI, 0.39-0.66), but VT below 8 ml/kg and PEEP greater than or equal to 5 cm H2O were not.
Conclusions: The authors identified an intraoperative lung-protective ventilation bundle as independently associated with pulmonary complications after cardiac surgery. The findings offer insight into components of protective ventilation associated with adverse outcomes and may serve as targets for future prospective interventional studies investigating the impact of specific protective ventilation strategies on postoperative outcomes after cardiac surgery.
Conflict of interest statement
Figures

Comment in
-
Lung-protective Ventilation in Cardiac Surgery: Comment.Anesthesiology. 2020 Jun;132(6):1610-1611. doi: 10.1097/ALN.0000000000003292. Anesthesiology. 2020. PMID: 32287044 No abstract available.
-
Lung-protective Ventilation in Cardiac Surgery: Reply.Anesthesiology. 2020 Jun;132(6):1611-1613. doi: 10.1097/ALN.0000000000003294. Anesthesiology. 2020. PMID: 32287045 Free PMC article. No abstract available.
-
Lung-protective Ventilation in Cardiac Surgery: Comment.Anesthesiology. 2020 Jun;132(6):1611. doi: 10.1097/ALN.0000000000003293. Anesthesiology. 2020. PMID: 32287046 No abstract available.
References
-
- Zochios V, Klein AA, Gao F: Protective Invasive Ventilation in Cardiac Surgery: A Systematic Review With a Focus on Acute Lung Injury in Adult Cardiac Surgical Patients. J Cardiothorac Vasc Anesth 2017 - PubMed
-
- Ibanez J, Riera M, Amezaga R, Herrero J, Colomar A, Campillo-Artero C, Ibarra JI de, Bonnin O: Long-Term Mortality After Pneumonia in Cardiac Surgery Patients: A Propensity-Matched Analysis. J Intensive Care Med 2016; 31:34–40 - PubMed
-
- Brown PP, Kugelmass AD, Cohen DJ, Reynolds MR, Culler SD, Dee AD, Simon AW: The frequency and cost of complications associated with coronary artery bypass grafting surgery: results from the United States Medicare program. Ann Thorac Surg 2008; 85:1980–6 - PubMed
-
- Garcia-Delgado M, Navarrete-Sanchez I, Colmenero M: Preventing and managing perioperative pulmonary complications following cardiac surgery. Curr Opin Anaesthesiol 2014; 27:146–52 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
