

The accuracy of lung auscultation in the practice of physicians and medical students
- PMID: 31404066
- PMCID: PMC6690530
- DOI: 10.1371/journal.pone.0220606
The accuracy of lung auscultation in the practice of physicians and medical students
Abstract
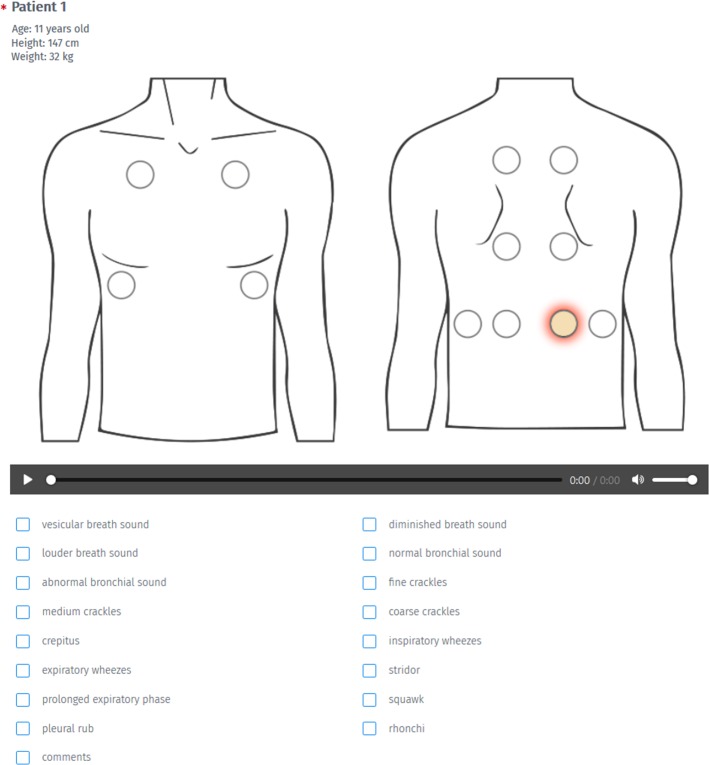
Background: Auscultation is one of the first examinations that a patient is subjected to in a GP's office, especially in relation to diseases of the respiratory system. However it is a highly subjective process and depends on the physician's ability to interpret the sounds as determined by his/her psychoacoustical characteristics. Here, we present a cross-sectional assessment of the skills of physicians of different specializations and medical students in the classification of respiratory sounds in children.
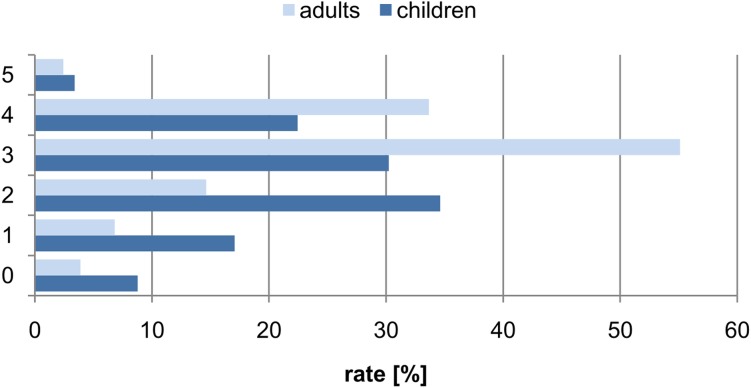
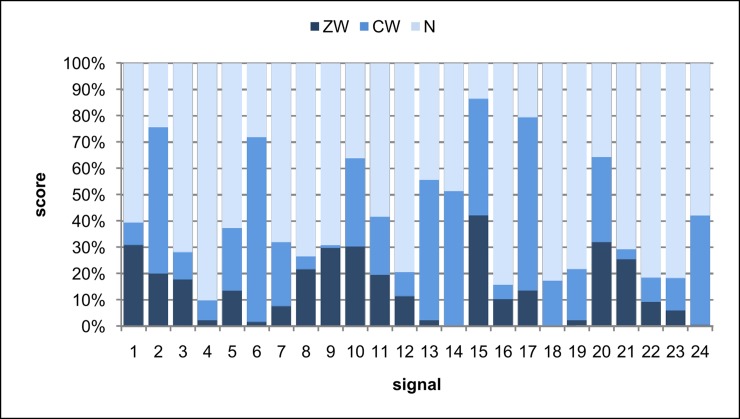
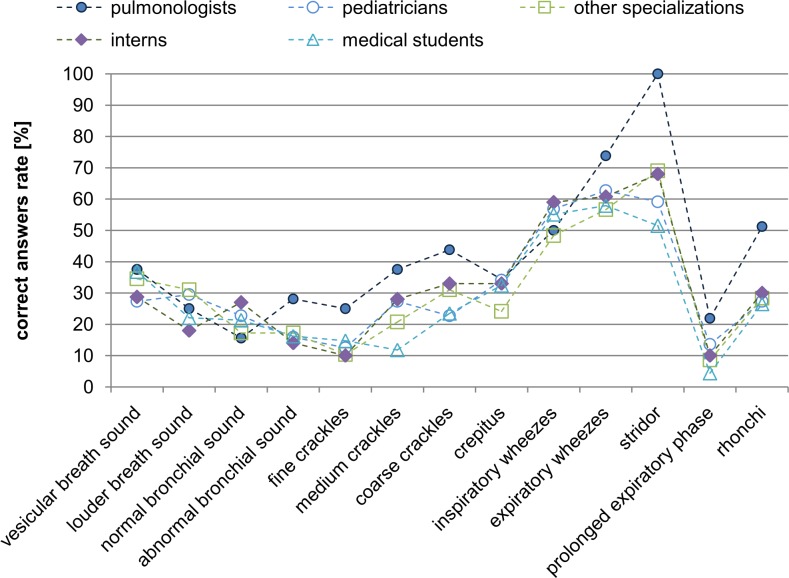
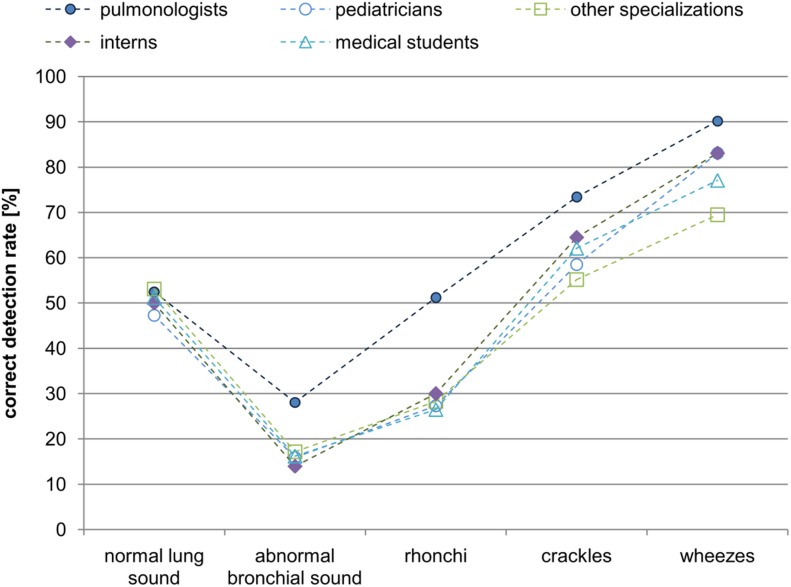
Methods and findings: 185 participants representing different medical specializations took part in the experiment. The experiment comprised 24 respiratory system auscultation sounds. The participants were tasked with listening to, and matching the sounds with provided descriptions of specific sound classes. The results revealed difficulties in both the recognition and description of respiratory sounds. The pulmonologist group was found to perform significantly better than other groups in terms of number of correct answers. We also found that performance significantly improved when similar sound classes were grouped together into wider, more general classes.
Conclusions: These results confirm that ambiguous identification and interpretation of sounds in auscultation is a generic issue which should not be neglected as it can potentially lead to inaccurate diagnosis and mistreatment. Our results lend further support to the already widespread acknowledgment of the need to standardize the nomenclature of auscultation sounds (according to European Respiratory Society, International Lung Sounds Association and American Thoracic Society). In particular, our findings point towards important educational challenges in both theory (nomenclature) and practice (training).
Conflict of interest statement
Honorata Hafke-Dys and Jędrzej Kociński are employed by both Adam Mickiewicz University in Poznań and the company StethoMe, and are shareholders of StethoMe. Adam Biniakowski is employed by StethoMe. Anna Bręborowicz is the StethoMe content consultant and coordinated the recordings at the hospital. All the authors were paid for their work. This does not alter our adherence to the PLOS ONE policies on sharing data and materials, and the results were obtained with all the required ethical standards and objectivity. It must be emphasized that StethoMe was established because we obtained the results presented in the manuscript and sought to change the status quo in this area of examination. This research was first inspired by the everyday situation in a GP’s office encountered by Honorata Hafke-Dys, Kociński and their children, and then by literature research and cooperation with: prof. Anna Bręborowicz from the Karol Jonscher Clinical Hospital in Poznań; Poznań University of Medical Sciences; and physicians from the Department of Pediatric Pneumonology, Allergology and Clinical Immunology.
Figures
References
-
- Francis NA, Melbye H, Kelly MJ, Cals JW, Hopstaken RM, Coenen S, et al. Variation in family physicians’ recording of auscultation abnormalities in patients with acute cough is not explained by case mix. A study from 12 European networks. European Journal of General Practice. 2013;19(2):77–84. 10.3109/13814788.2012.733690 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
