

Open adrenalectomy
- PMID: 31404196
- PMCID: PMC6646811
- DOI: 10.21037/gs.2019.05.10
Open adrenalectomy
Abstract
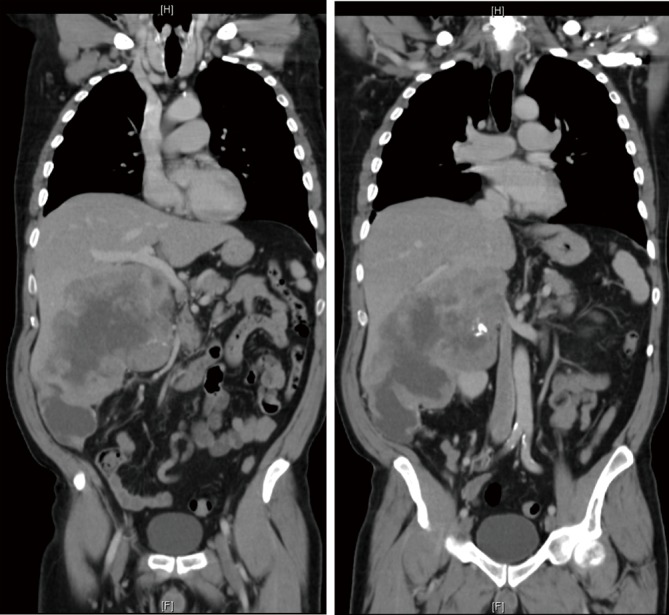
In an era when minimally invasive adrenalectomy is the gold standard treatment for majority of patients presenting with adrenal tumours, open adrenalectomy has become an operation that should be centralised in regional referral centers. Its main indication is represented by patients with large (>8 cm) phaeochromocytomas and patients with cortical adrenal tumours suspected of malignancy either because of their size (>4-6 cm) or because of radiological appearance of local invasion. Based on local expertise some of these patients might benefit from multidisciplinary input from liver or transplant surgeons. This chapter will discuss the anatomical landmarks and will comment on different steps in the procedure for right- or left-sided procedure. It is outside the scope of this chapter to settle the ongoing debate about patient selection for laparoscopic or open adrenalectomy when the diagnosis of adrenocortical cancer is suspected preoperatively.
Keywords: Adrenalectomy; surgical technique.
Conflict of interest statement
Conflicts of Interest: The author has no conflicts of interest to declare.
Figures
References
-
- Welbourn B. The History of Endocrine Surgery. New York: Praeger, 1990:147.
-
- Cahill GF. Hormonal tumours of the adrenals. Surgery 1944;16:233.
-
- Young HH. Genital abnormalities: Hermaphroditism and related adrenal disease. Baltimore: Williams & Wilkins, 1937.
-
- Fassnacht M, Dekkers OM, Else T, et al. European Society of Endocrinology Clinical Practice Guidelines on the management of adrenocortical carcinoma in adults, in collaboration with the European Network for the Study of Adrenal Tumors. Eur J Endocrinol 2018;179:G1-G46. 10.1530/EJE-18-0608 - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources