

Eosinophil Inflammation and Hyperresponsiveness in the Airways as Phenotypes of COPD, and Usefulness of Inhaled Glucocorticosteroids
- PMID: 31404293
- PMCID: PMC6676333
- DOI: 10.3389/fphar.2019.00765
Eosinophil Inflammation and Hyperresponsiveness in the Airways as Phenotypes of COPD, and Usefulness of Inhaled Glucocorticosteroids
Abstract
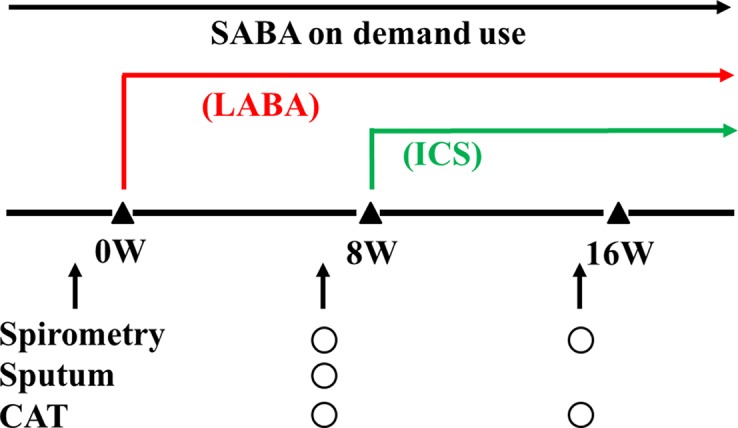
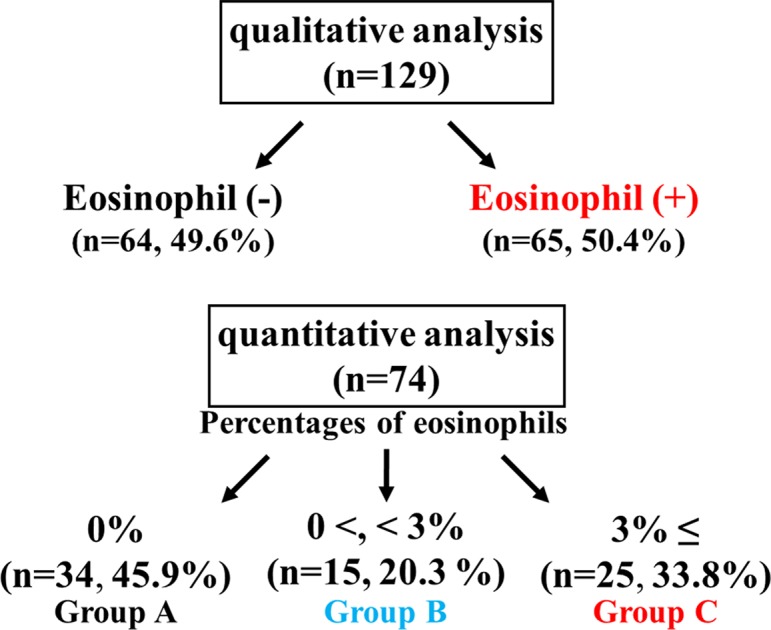
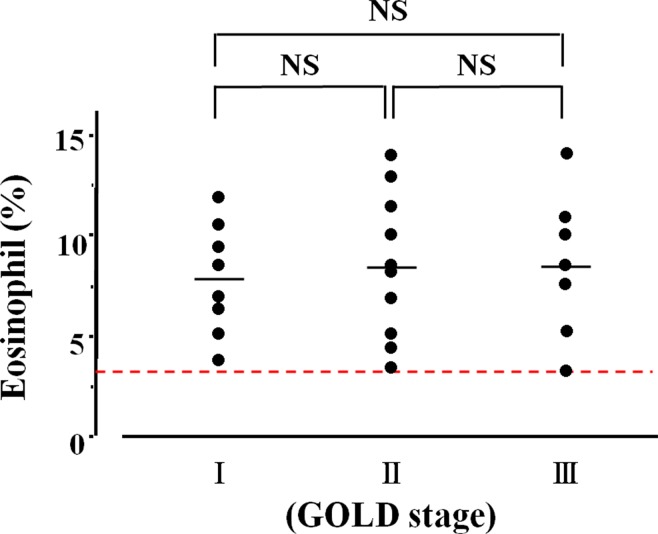
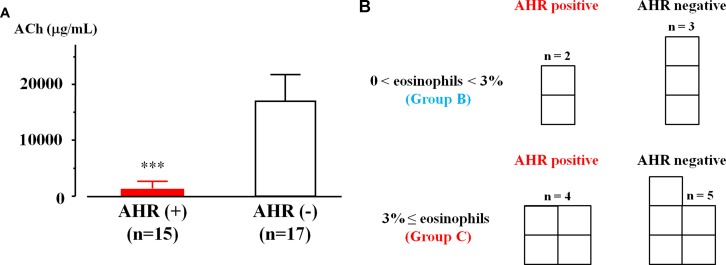
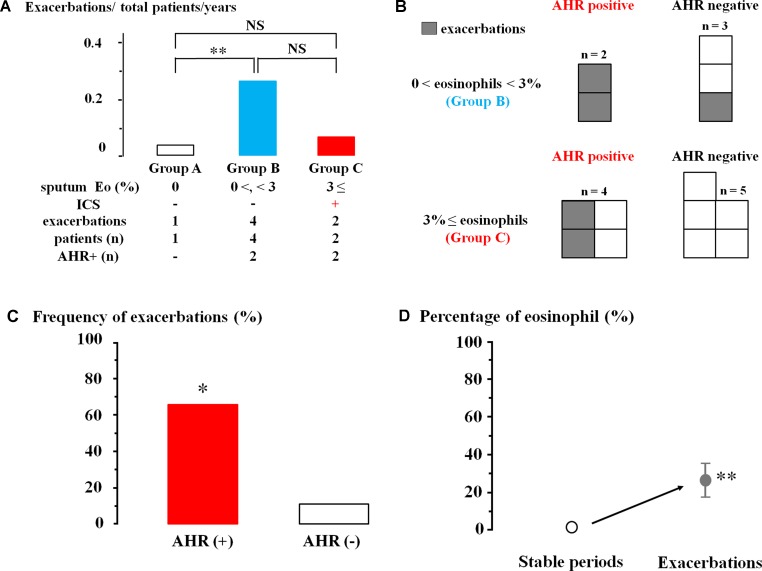
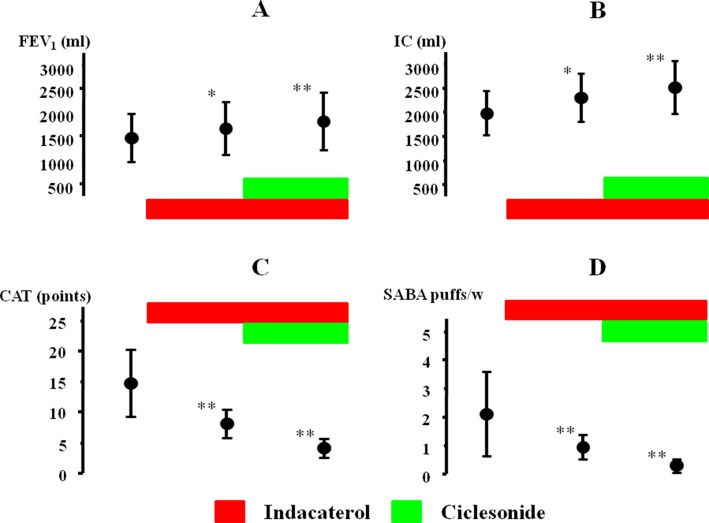
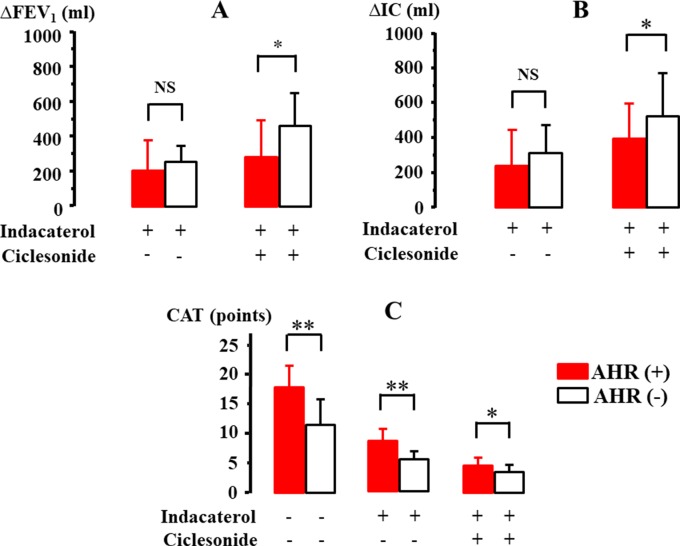
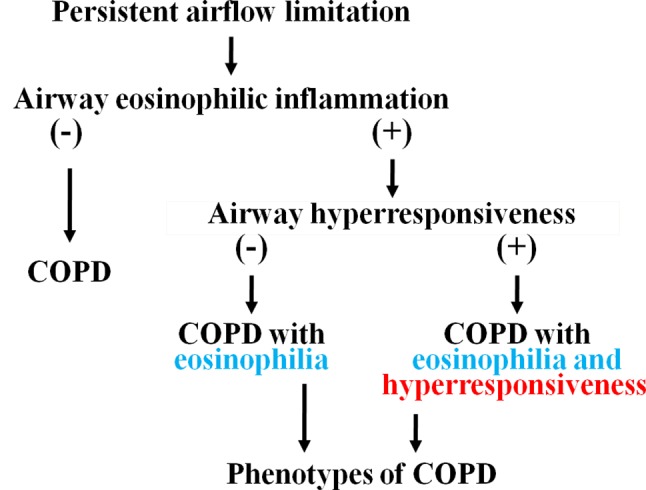
Background: The differential diagnosis in persistent airway limitation is sometimes not so clear in older adults. Airway eosinophilia and airway hyperresponsiveness may develop in some cases with chronic obstructive lung disease (COPD), independent of asthma. However, little is known about clinical significance of these phenotypes of COPD in detail. Aims and objectives: This clinical study was designed to examine prevalence of airway eosinophilia and airway hyperresponsiveness in COPD who have no symptom and no past history of asthma, and to examine involvement of these pathophysiological features of asthma in the management and therapy for COPD. Methods: Sputum examination via qualitative and quantitative procedures was performed in stable COPD (GOLD 1-3). When sputum eosinophils were qualitatively (≥+) or quantitatively assessed (≥3%), ciclesonide (inhaled glucocorticosteroids) was added on bronchodilators. In cases with FEV1 ≥ 70% of predicted values, acetylcholine provocation test was examined for assessment of airway hyperresponsiveness. Therapeutic effect was evaluated using spirometry and COPD assessment test (CAT). Results: Sputum eosinophils were observed in 65 (50.4%) of 129 subjects using qualitative analysis; in contrast, lower grade (>0%) and higher grade (≥3%) were observed in 15 (20.3%) and 25 (33.8%) of 74 subjects using quantitative analysis. Airway hyperresponsiveness developed in 46.9% of these subjects with sputum eosinophils. Exacerbations occurred much more frequently in lower-grade airway eosinophilia without ciclesonide than in higher-grade airway eosinophilia with ciclesonide. Airway hyperresponsiveness significantly increased frequency of exacerbations in COPD with both lower and higher grade in airway eosinophilia. Addition of ciclesonide to indacaterol markedly improved lung function (FEV1, IC), CAT score, and reliever use in these subjects with airway eosinophilia determined by qualitative analysis. However, ciclesonide was less effective in improving these values in subjects with airway hyperresponsiveness than in those without airway hyperresponsiveness. Conclusions: Airway eosinophilia and airway hyperresponsiveness are complicated with 25-50% of COPD that have no symptom and history for asthma. These phenotypes of COPD are closely related to symptom stability and reactivity to glucocorticosteroids. These phenotypes may play key roles for advancement of the management and therapy of this disease.
Keywords: LABA; airway eosinophil inflammation; asthma-COPD overlap; bronchial hyperreactivity; sputum examination.
Figures
References
LinkOut - more resources
Full Text Sources
Miscellaneous