

NeoDoppler: New ultrasound technology for continous cerebral circulation monitoring in neonates
- PMID: 31404920
- PMCID: PMC6960092
- DOI: 10.1038/s41390-019-0535-0
NeoDoppler: New ultrasound technology for continous cerebral circulation monitoring in neonates
Abstract
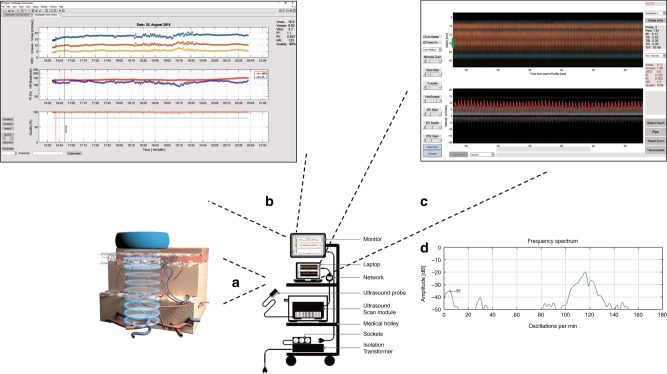
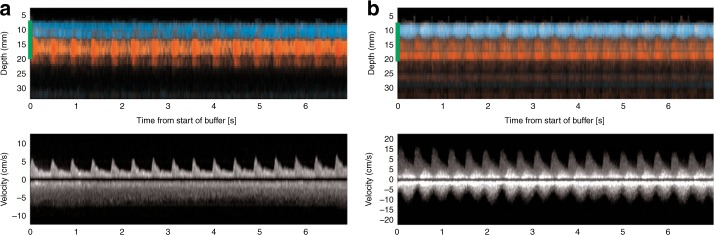
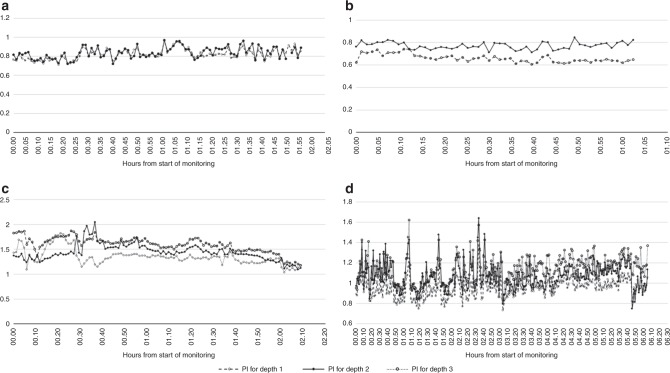
Background: There is a strong need for continuous cerebral circulation monitoring in neonatal care, since suboptimal cerebral blood flow may lead to brain injuries in preterm infants and other critically ill neonates. NeoDoppler is a novel ultrasound system, which can be gently fixed to the anterior fontanel and measure cerebral blood flow velocity continuously in different depths of the brain simultaneously. We aimed to study the feasibility, accuracy, and potential clinical applications of NeoDoppler in preterm infants and sick neonates.
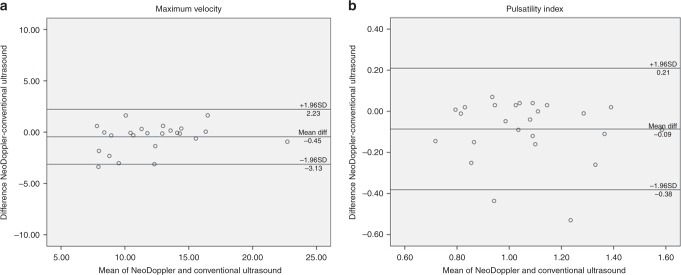
Method: Twenty-five infants born at different gestational ages with a variety of diagnoses on admission were included. The probe was placed over the anterior fontanel, and blood flow velocity data were continuously recorded. To validate NeoDoppler, we compared the measurements with conventional ultrasound; agreement was assessed using Bland-Altman plots.
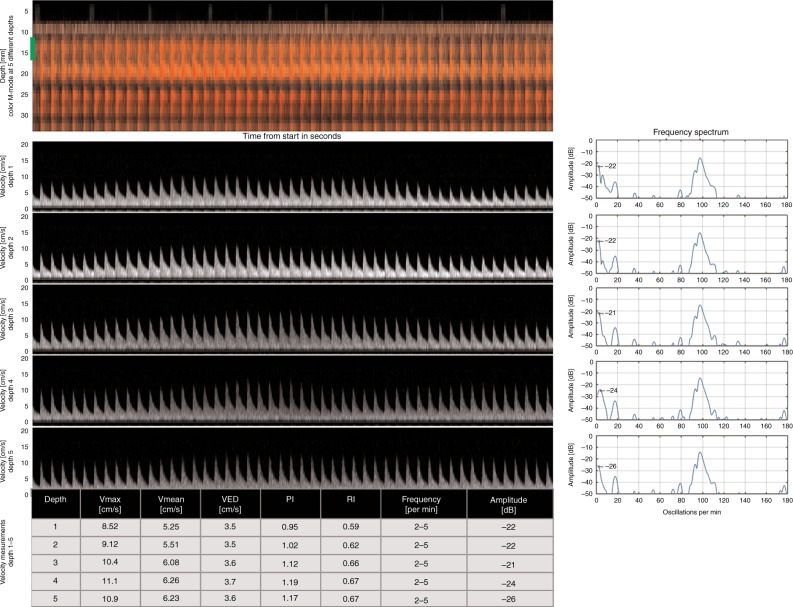
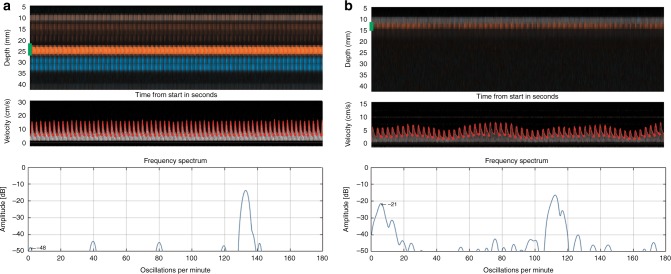
Results: NeoDoppler can provide accurate and continuous data on cerebral blood flow velocity in several depths simultaneously. Limits of agreement between the measurements obtained with the two methods were acceptable.
Conclusion: By monitoring the cerebral circulation continuously, increased knowledge of cerebral hemodynamics in preterm infants and sick neonates may be acquired. Improved monitoring of these vulnerable brains during a very sensitive period of brain development may contribute toward preventing brain injuries.
Conflict of interest statement
NTNU and St. Olavs Hospital, Trondheim University Hospital may benefit financially from commercialization of the ultrasound equipment through future possible intellectual properties; this may include financial benefits to authors of this article. S.D.V., H.T., R.S. and S.A.N. are co-inventors of NeoDoppler. T.F. declares no competing interests.
Figures
Similar articles
-
Effects of tilt on cerebral hemodynamics measured by NeoDoppler in healthy neonates.Pediatr Res. 2021 Oct;90(4):888-895. doi: 10.1038/s41390-020-01354-w. Epub 2021 Jan 27. Pediatr Res. 2021. PMID: 33504967 Free PMC article.
-
Cerebral blood flow dynamics during cardiac surgery in infants.Pediatr Res. 2025 Feb;97(2):625-633. doi: 10.1038/s41390-024-03161-z. Epub 2024 Apr 3. Pediatr Res. 2025. PMID: 38570558 Free PMC article.
-
Point-of-care brain ultrasound and transcranial doppler or color-coded doppler in critically ill neonates and children.Eur J Pediatr. 2024 Mar;183(3):1059-1072. doi: 10.1007/s00431-023-05388-0. Epub 2023 Dec 19. Eur J Pediatr. 2024. PMID: 38112802 Review.
-
[Clinical study of neonatal cardiac output measurement methods].Zhonghua Er Ke Za Zhi. 2013 Jan;51(1):58-63. Zhonghua Er Ke Za Zhi. 2013. PMID: 23527933 Chinese.
-
[Approach by neuroimaging with power flow Doppler imaging].No To Hattatsu. 2002 Mar;34(2):147-52. No To Hattatsu. 2002. PMID: 11905011 Review. Japanese.
Cited by
-
Transfontanelle photoacoustic imaging: ultrasound transducer selection analysis.Biomed Opt Express. 2022 Jan 10;13(2):676-693. doi: 10.1364/BOE.446087. eCollection 2022 Feb 1. Biomed Opt Express. 2022. PMID: 35284180 Free PMC article.
-
Hands-free continuous carotid Doppler ultrasound for detection of the pulse during cardiac arrest in a porcine model.Resusc Plus. 2023 Jun 20;15:100412. doi: 10.1016/j.resplu.2023.100412. eCollection 2023 Sep. Resusc Plus. 2023. PMID: 37448689 Free PMC article.
-
Continuous cerebral blood flow monitoring: What should we do with these extra numbers?BJA Open. 2023 Jun 23;7:100148. doi: 10.1016/j.bjao.2023.100148. eCollection 2023 Sep. BJA Open. 2023. PMID: 37638084 Free PMC article.
-
Neurosonography: Shaping the future of neuroprotection strategies in extremely preterm infants.Heliyon. 2024 May 24;10(11):e31742. doi: 10.1016/j.heliyon.2024.e31742. eCollection 2024 Jun 15. Heliyon. 2024. PMID: 38845994 Free PMC article. Review.
-
Chest Compression in Neonatal Cardiac Arrest: Cerebral Blood Flow Measurements in Experimental Models.Healthcare (Basel). 2020 Jan 10;8(1):17. doi: 10.3390/healthcare8010017. Healthcare (Basel). 2020. PMID: 32284508 Free PMC article. Review.
References
-
- Volpe JJ. Brain injury in the premature infant-from pathogenesis to prevention. Brain Dev. 1997;19:519–534. - PubMed
-
- Watkins AM, West CR, Cooke RW. Blood pressure and cerebral haemorrhage and ischaemia in very low birthweight infants. Early Hum. Dev. 1989;19:103–110. - PubMed
-
- Bolisetty S, et al. Intraventricular hemorrhage and neurodevelopmental outcomes in extreme preterm infants. Pediatrics. 2014;133:55–62. - PubMed
-
- Jarjour IT. Neurodevelopmental outcome after extreme prematurity: a review of the literature. Pediatr. Neurol. 2015;52:143–152. - PubMed
-
- Dempsey EM, Al Hazzani F, Barrington KJ. Permissive hypotension in the extremely low birthweight infant with signs of good perfusion. Arch. Dis. Child. Fetal Neonatal Ed. 2009;94:F241–F244. - PubMed
