

The Benefits of Oral Rehydration on Orthostatic Intolerance in Children with Postural Tachycardia Syndrome
- PMID: 31405524
- PMCID: PMC6815702
- DOI: 10.1016/j.jpeds.2019.07.041
The Benefits of Oral Rehydration on Orthostatic Intolerance in Children with Postural Tachycardia Syndrome
Abstract
Objective: To evaluate whether equal volumes of oral rehydration solution (ORS) or intravenous (IV) saline provide similar improvements in cardiovascular status during controlled orthostatic challenge when administered to subjects with postural tachycardia syndrome (POTS) with orthostatic intolerance.
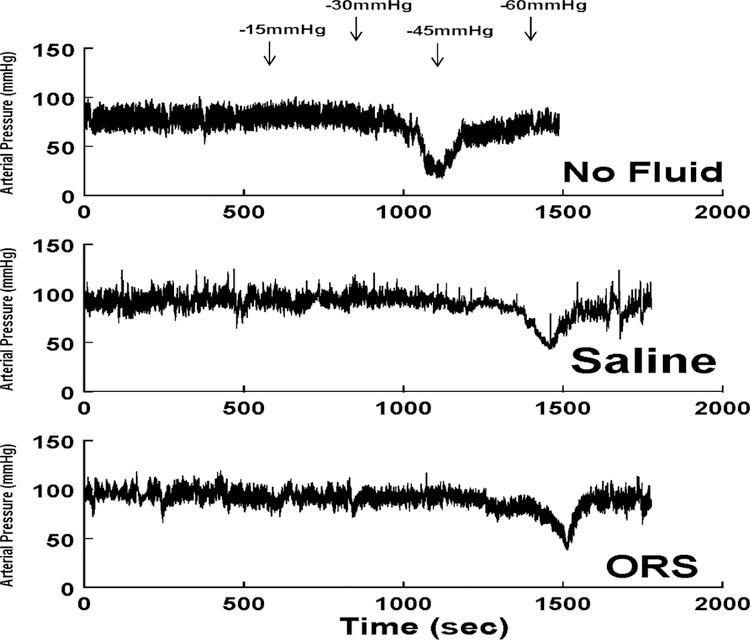
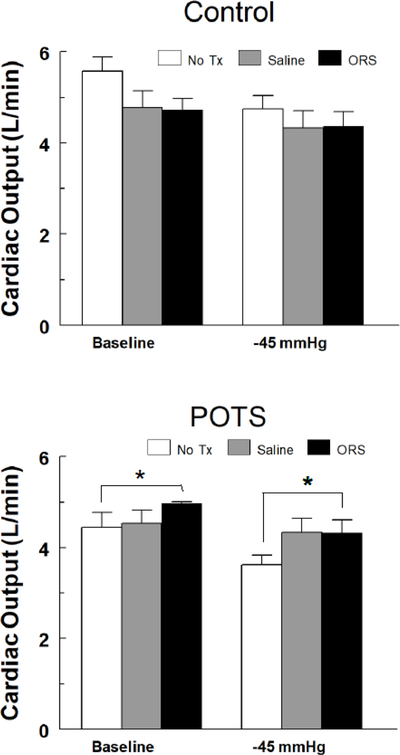
Study design: We studied the neurovascular response to fluid loading during orthostatic stress using lower body negative pressure (LBNP) in 10 subjects with POTS with orthostatic intolerance and 15 controls, and on subsequent days before and 1 hour after IV saline infusion or ingestion of ORS.
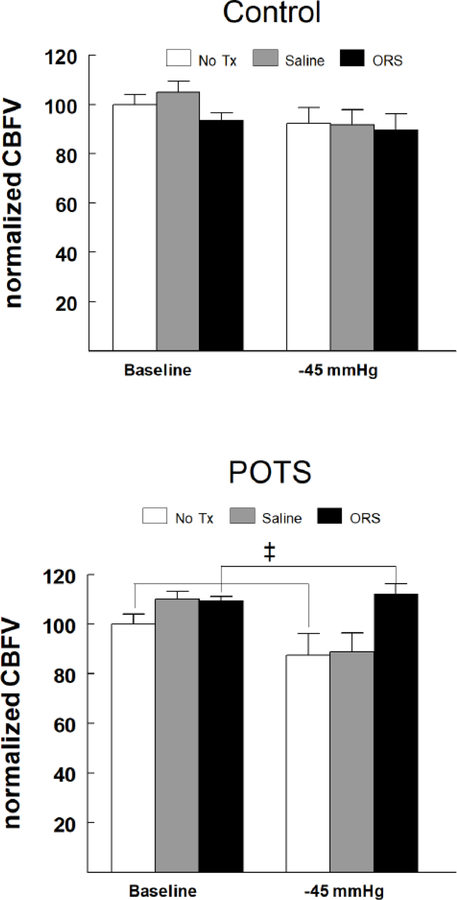
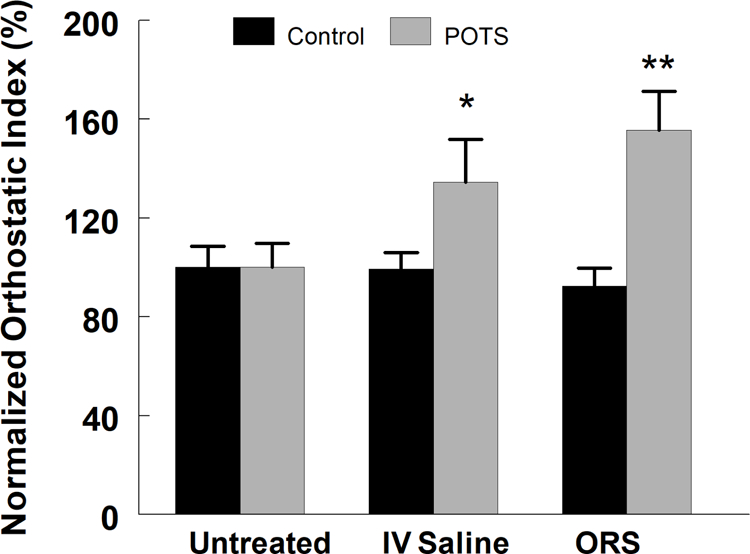
Results: Subjects with POTS exhibited reduced tolerance to LBNP (P < .0001) compared with controls (Orthostatic Index of 35 715 ± 3469 vs 93 980 ± 7977, respectively). In POTS, following ORS but not saline infusion, cerebral blood flow velocity (CBFv) was significantly higher than that with no treatment, at -45 mm Hg (P < .0005). Although fluid loading did not confer any advantage in controls, subjects with POTS experienced a significant improvement in orthostatic tolerance following both saline infusion (100 ± 9.7 vs 134.5 ± 17.4; P < .05) and ORS (100 ± 9.7 vs 155.6 ± 15.7; P < .001) when evaluated by normalized orthostatic index (P < .001, compared with untreated baseline).
Conclusions: Maintenance of CBFv may have resulted in the improved short-term orthostatic tolerance exhibited by the subjects with POTS following ORS administration. ORS is a convenient, safe, and effective therapy for short-term relief of orthostatic intolerance.
Copyright © 2019 Elsevier Inc. All rights reserved.
Figures
References
-
- Sheriff DD, Nadland IH, Toska K. Role of sympathetic responses on the hemodynamic consequences of rapid changes in posture in humans. J Appl Physiol (1985 ) 2010;108:523–532. - PubMed
-
- Brack KE, Coote JH, Ng GA. Vagus nerve stimulation inhibits the increase in Ca2+ transient and left ventricular force caused by sympathetic nerve stimulation but has no direct effects alone--epicardial Ca2+ fluorescence studies using fura-2 AM in the isolated innervated beating rabbit heart. Exp Physiol 2010;95:80–92. - PubMed
-
- Raczak G, La Rovere MT, Mortara A, Assandri J, Prpa A, Pinna GD, et al. Arterial baroreflex modulation of heart rate in patients early after heart transplantation: lack of parasympathetic reinnervation. J Heart Lung Transplant 1999;18:399–406. - PubMed
-
- Toda N, Ayajiki K, Okamura T. Cerebral blood flow regulation by nitric oxide: recent advances. Pharmacol Rev 2009;61:62–97. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
