

Nationwide trends in drug-coated balloon and drug-eluting stent utilization in the femoropopliteal arteries
- PMID: 31405761
- PMCID: PMC7007839
- DOI: 10.1016/j.jvs.2019.05.034
Nationwide trends in drug-coated balloon and drug-eluting stent utilization in the femoropopliteal arteries
Abstract
Objective: Drug-coated balloons (DCB) and drug-eluting stents (DES) have significantly altered treatment paradigms for femoropopliteal lesions. We aimed to describe changes in practice patterns as a result of the infusion of these technologies into the treatment of peripheral arterial disease.
Methods: We queried the Vascular Quality Initiative registry from 2010 to 2017 for all peripheral vascular interventions involving the superficial femoral artery and/or the popliteal artery. Cases were divided into a PRE and a POST era with a cutoff of September 2016, when specific device identity was first recorded in Vascular Quality Initiative. For each artery, a primary treatment was identified as either plain balloon angioplasty, atherectomy, DCB, bare-metal stent, or DES. The relative distribution of primary treatments between the PRE and POST eras was evaluated, as were lesion characteristics associated with DCB and DES use and regional variability in the adoption of these new technologies.
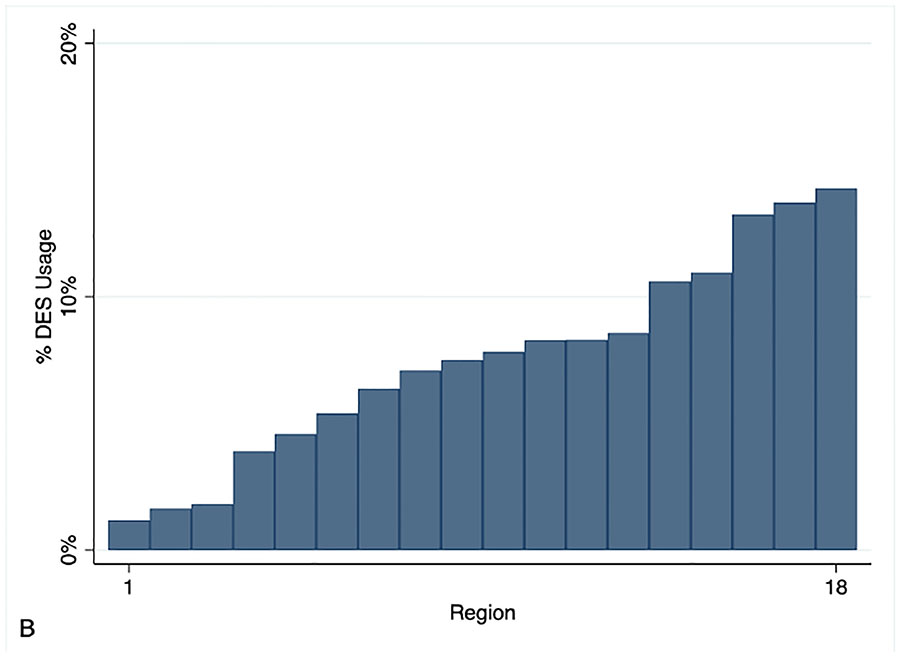
Results: Of 210,666 arteries in the dataset, 91,864 femoropopliteal arteries (across 74,842 procedures in 55,437 patients) were included. Each artery received 1.5 ± 0.6 treatments. Primary treatment use changed from 40% balloon angioplasty, 45% stenting, and 15% atherectomy in the PRE era to 22% plain balloon angioplasty, 26% bare-metal stent, 8% atherectomy, 37% DCB, and 8% DES in the POST era (P < .001). Forty-three percent of arteries received a drug-containing device as a primary or adjunctive therapy and 1.3% received both a DCB and DES in the POST era. DCB use as the primary treatment was highest in lesions with length 10.0 to 19.9 cm (42%), TransAtlantic InterSociety A, B, or C lesions (38%), and lesions with mild to no calcification (38%). DES use was highest in lesions with a length of 20 cm or more (12%), TransAtlantic InterSociety D lesions (13%), and lesions with moderate to severe calcification (9%). The range of use across 18 regions was 125 to 40% for DCB and 1% to 14% for DES. Regional variability was greater for DES (SD 4% vs mean 8%) than for DCB (SD 7% vs mean 29%).
Conclusions: There has been a rapid dissemination of DCB and DES technology in the femoropopliteal vessels, with nearly one-half of arteries receiving a drug-containing therapy in modern practice. DCBs are most used in medium length, minimally calcified lesions and DESs are most used in longer, more heavily calcified lesions. There is significant regional variability in adoption, especially with DES.
Keywords: Drug-coated balloons; Drug-eluting stents; Femoropopliteal; Trends.
Copyright © 2019 Society for Vascular Surgery. Published by Elsevier Inc. All rights reserved.
Figures






References
-
- Criqui MH, Aboyans V. Epidemiology of peripheral artery disease. Circ Res. 2015;116(9):1509–26. - PubMed
-
- Conte MS, Pomposelli FB. Society for Vascular Surgery Practice guidelines for atherosclerotic occlusive disease of the lower extremities management of asymptomatic disease and claudication. Introduction. J Vasc Surg. 2015;61(3 Suppl):1S. - PubMed
-
- Norgren L, Hiatt WR, Dormandy JA, Nehler MR, Harris KA, Fowkes FG, et al. Inter-Society Consensus for the Management of Peripheral Arterial Disease (TASC II). J Vasc Surg. 2007;45 Suppl S:S5–67. - PubMed
-
- Baril DT, Chaer RA, Rhee RY, Makaroun MS, Marone LK. Endovascular interventions for TASC II D femoropopliteal lesions. J Vasc Surg. 2010;51(6):1406–12. - PubMed
-
- Krankenberg H, Schluter M, Steinkamp HJ, Burgelin K, Scheinert D, Schulte KL, et al. Nitinol stent implantation versus percutaneous transluminal angioplasty in superficial femoral artery lesions up to 10 cm in length: the femoral artery stenting trial (FAST). Circulation. 2007;116(3):285–92. - PubMed
