

High Cervical Lateral Approach to Safely Remove the Cystic Retro-odontoid Pseudotumor: Technical Note
- PMID: 31406052
- PMCID: PMC6796063
- DOI: 10.2176/nmc.tn.2019-0060
High Cervical Lateral Approach to Safely Remove the Cystic Retro-odontoid Pseudotumor: Technical Note
Abstract
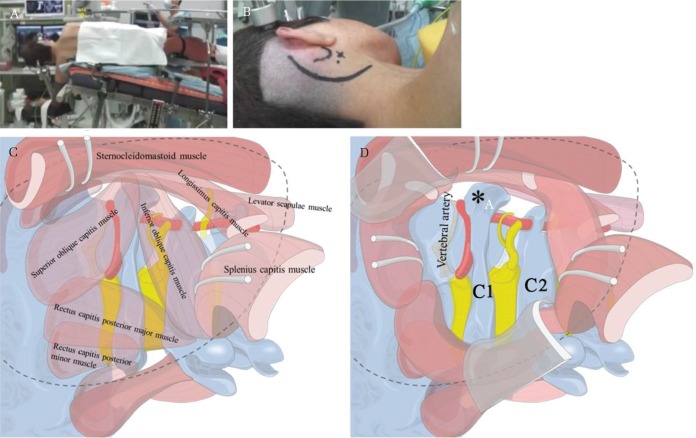
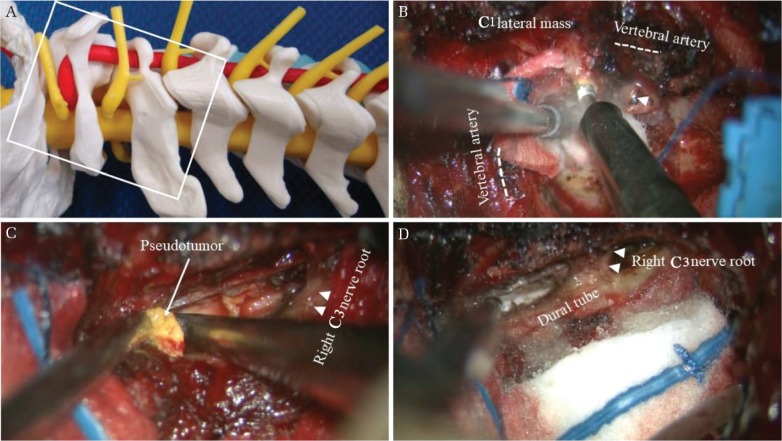
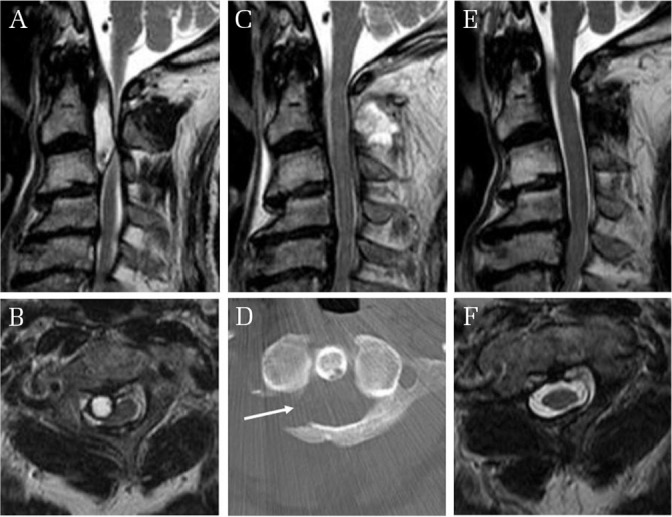
Surgery for neoplastic or vascular lesions at the craniovertebral junction remains one of the major challenges for neurosurgeons, because of issues such as the complex functional anatomy and vascular structures. We present three cases in which the high cervical lateral approach was used to safely remove the cystic retro-odontoid pseudotumor, not associated with rheumatoid arthritis, severely compressing the spinal cord. The mean age of patients was 74.7 years (range, 73-77 years). Neurological condition was assessed based on the neurosurgical cervical spine scale. A high cervical lateral approach was applied to remove the pseudotumor safely. Mean duration of follow-up after surgery was 21.3 months (range, 18-24 months). Mean recovery rate was 77.8%. All patients showed acceptable or satisfactory functional recovery, although one patient (Case 2) developed mild paralysis of the facial and spinal accessory nerve on the surgical approach side, but that completely recovered within about 1 month after surgery. Postoperative assessment at the recent follow-up suggested no significant aggravation of neck movement. This technical note suggests that the high cervical lateral approach can be considered as a surgical option for cystic retro-odontoid pseudotumor, not associated with rheumatoid arthritis, severely compressing the spinal cord. Safe management of the vertebral artery is one of the key considerations.
Keywords: atlantoaxial instability; high cervical lateral approach; retro-odontoid pseudotumor; spinal accessory nerve; vertebral artery.
Conflict of interest statement
No funds were received in support of this work. No benefits in any form have been or will be received from any commercial party related directly or indirectly to the subject of this manuscript. All authors report no conflicts of interest concerning the materials or methods used in this study or the findings specified in this paper. All authors who are members of The Japan Neurosurgical Society (JNS) have registered online Self-reported COI Disclosure Statement Forms through the website for JNS members.
Figures
References
-
- Spetzler RF, Hadley MN, Sonntag VK: The transoral approach to the anterior superior cervical spine. A review of 29 cases. Acta Neurochir Suppl (Wien) 43: 69–74, 1988 - PubMed
-
- Shucart WA, Klériga E: Lateral approach to the upper cervical spine. Neurosurgery 6: 278–281, 1980 - PubMed
-
- George B, Dematons C, Cophignon J: Lateral approach to the anterior portion of the foramen magnum. Application to surgical removal of 14 benign tumors: technical note. Surg Neurol 29: 484–490, 1988 - PubMed
-
- Sen CN, Sekhar LN: An extreme lateral approach to intradural lesions of the cervical spine and foramen magnum. Neurosurgery 27: 197–204, 1990 - PubMed