

Visual inputs and postural manipulations affect the location of somatosensory percepts elicited by electrical stimulation
- PMID: 31406122
- PMCID: PMC6690924
- DOI: 10.1038/s41598-019-47867-1
Visual inputs and postural manipulations affect the location of somatosensory percepts elicited by electrical stimulation
Abstract
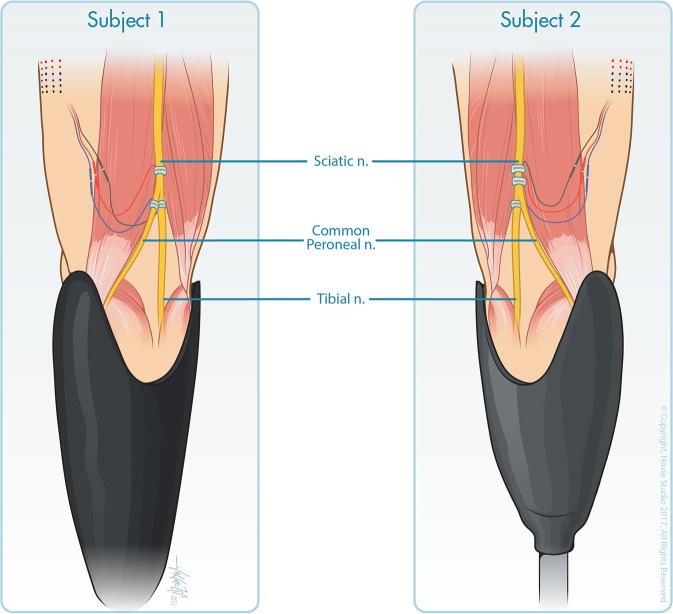
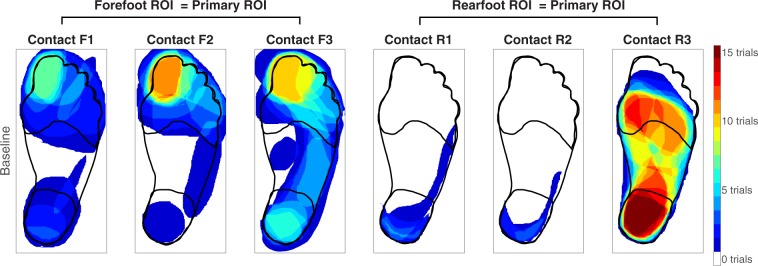
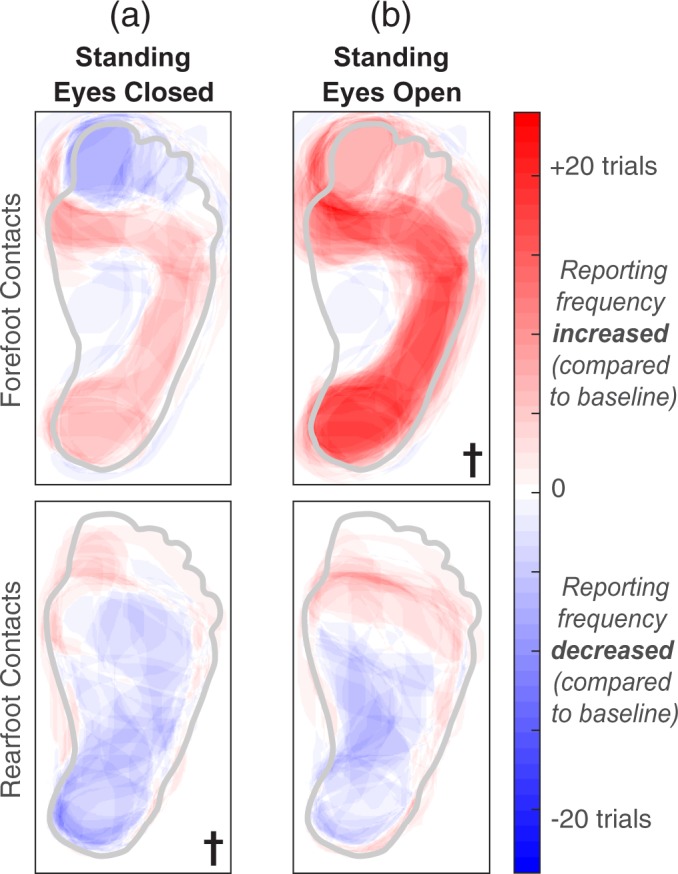
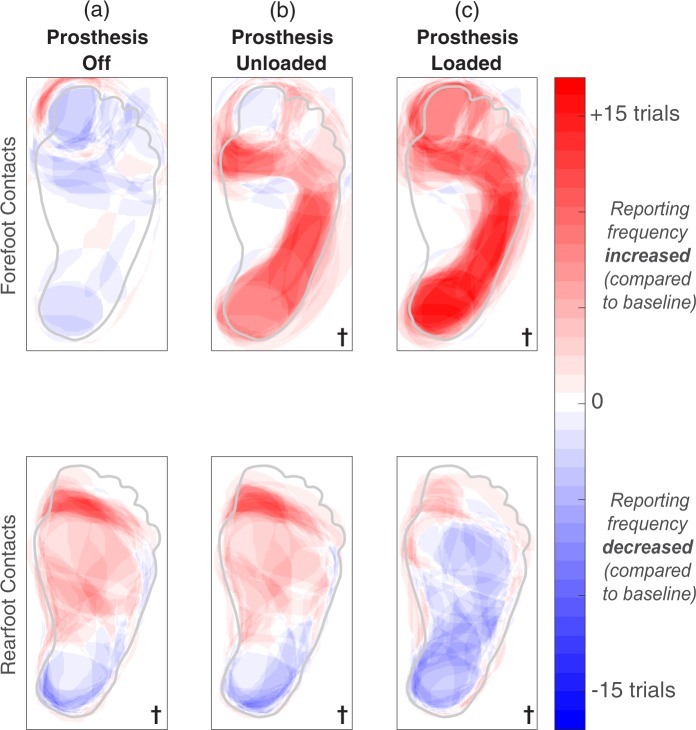
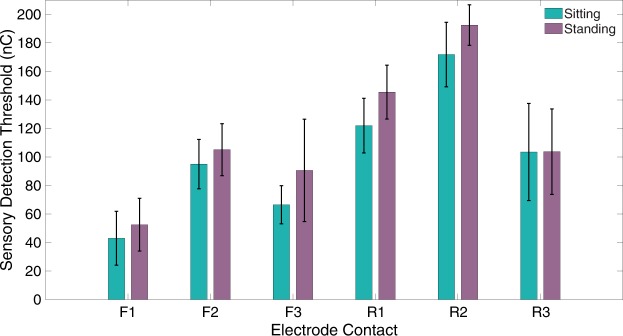
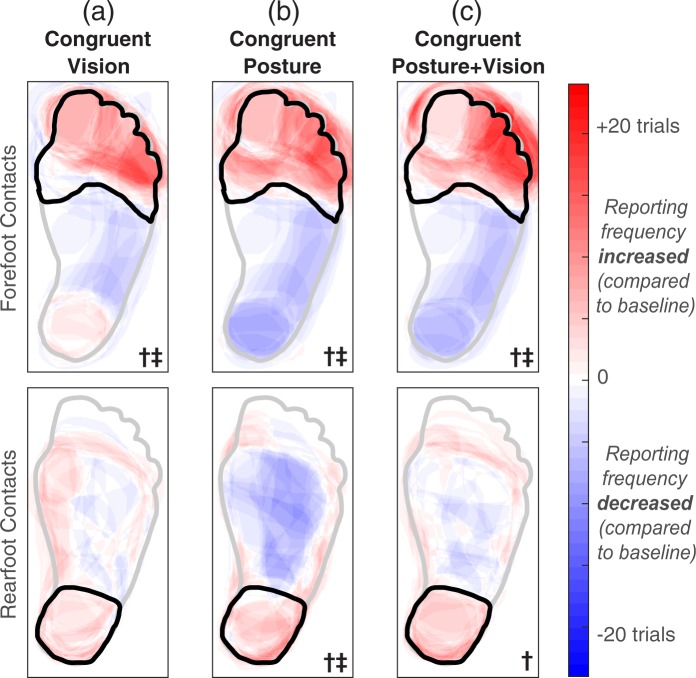
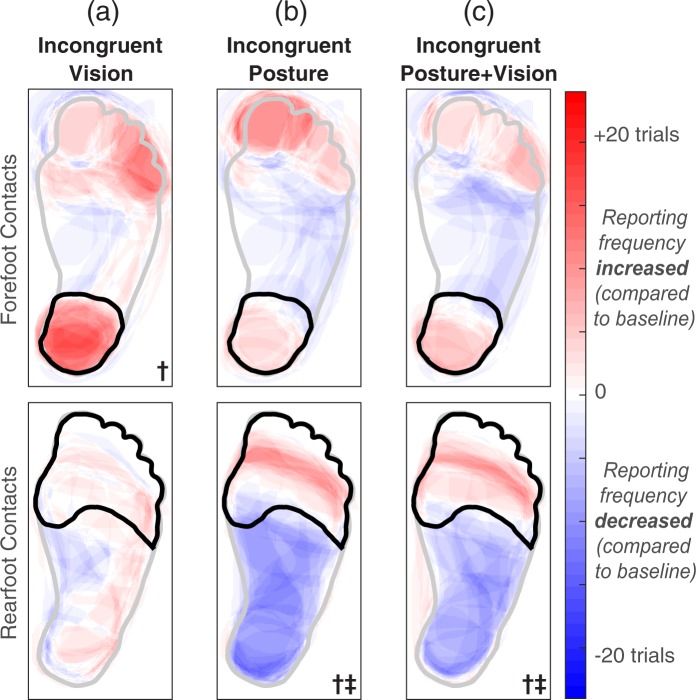
The perception of somatosensation requires the integration of multimodal information, yet the effects of vision and posture on somatosensory percepts elicited by neural stimulation are not well established. In this study, we applied electrical stimulation directly to the residual nerves of trans-tibial amputees to elicit sensations referred to their missing feet. We evaluated the influence of congruent and incongruent visual inputs and postural manipulations on the perceived size and location of stimulation-evoked somatosensory percepts. We found that although standing upright may cause percept size to change, congruent visual inputs and/or body posture resulted in better localization. We also observed visual capture: the location of a somatosensory percept shifted toward a visual input when vision was incongruent with stimulation-induced sensation. Visual capture did not occur when an adopted posture was incongruent with somatosensation. Our results suggest that internal model predictions based on postural manipulations reinforce perceived sensations, but do not alter them. These characterizations of multisensory integration are important for the development of somatosensory-enabled prostheses because current neural stimulation paradigms cannot replicate the afferent signals of natural tactile stimuli. Nevertheless, multisensory inputs can improve perceptual precision and highlight regions of the foot important for balance and locomotion.
Conflict of interest statement
The authors declare no competing interests.
Figures


References
-
- Perovic M. Electrical stimulation of the forearm. Journal of Automatic Control. 2013;21:13–18. doi: 10.2298/JAC1301013P. - DOI
-
- Crea S, Cipriani C, Donati M, Carrozza MC, Vitiello N. Providing Time-Discrete Gait Information by Wearable Feedback Apparatus for Lower-Limb Amputees: Usability and Functional Validation. IEEE Transactions on Neural Systems and Rehabilitation Engineering. 2015;23:250–257. doi: 10.1109/TNSRE.2014.2365548. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
