

Engineering patient-specific cancer immunotherapies
- PMID: 31406259
- PMCID: PMC6783331
- DOI: 10.1038/s41551-019-0436-x
Engineering patient-specific cancer immunotherapies
Abstract
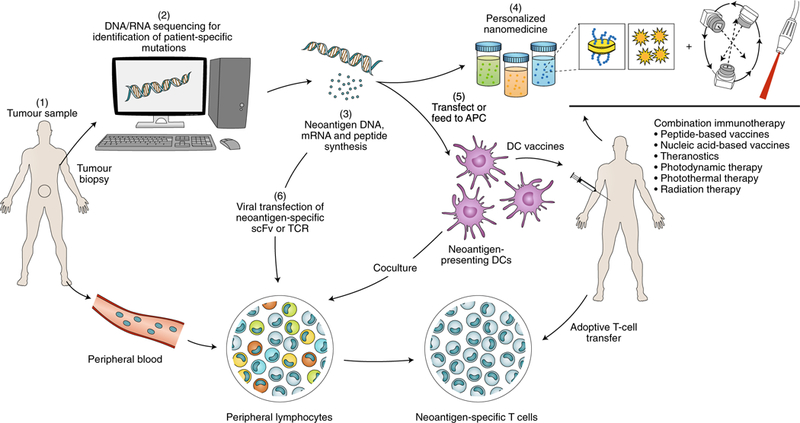
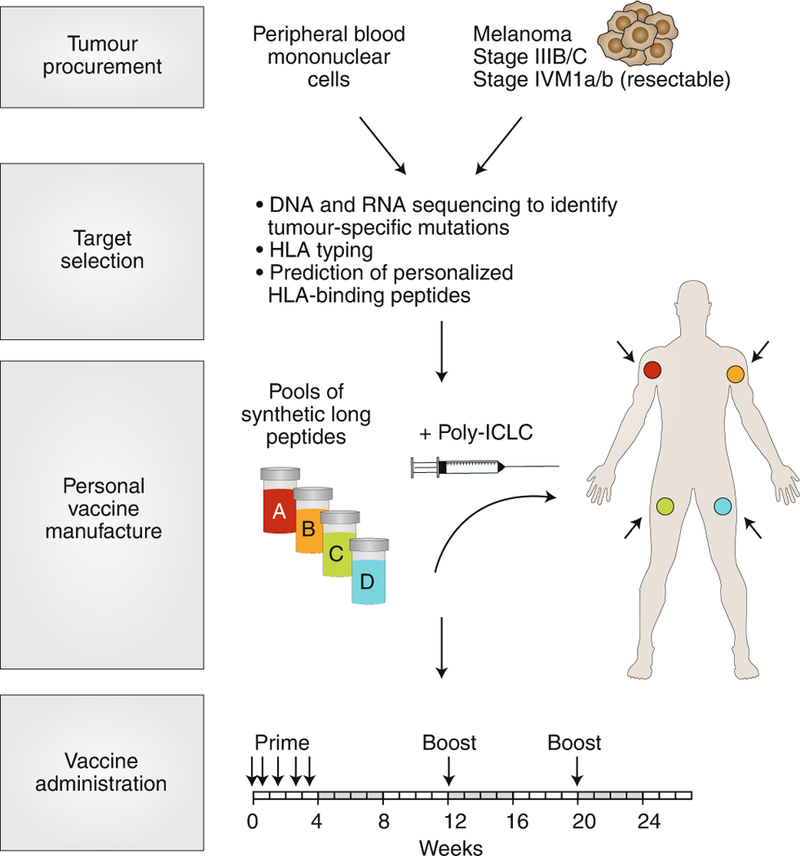
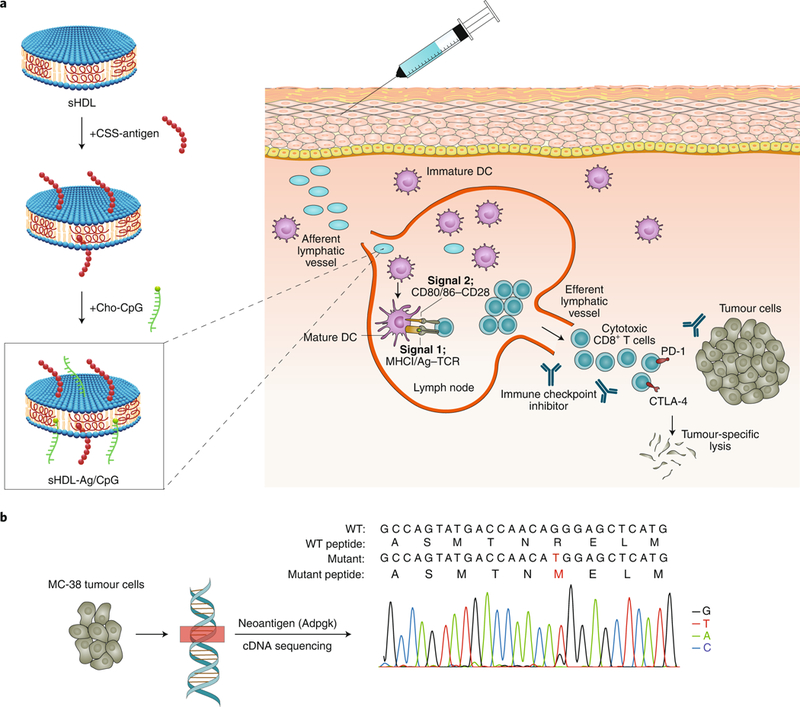
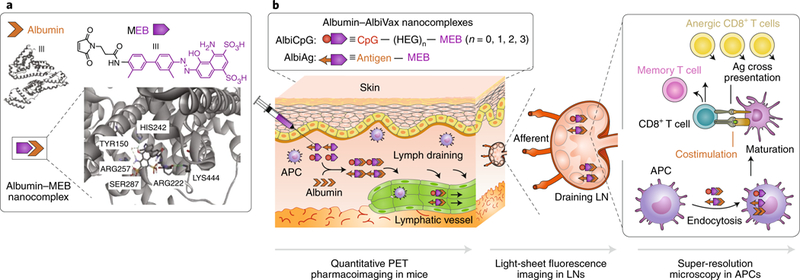
Research into the immunological processes implicated in cancer has yielded a basis for the range of immunotherapies that are now considered the fourth pillar of cancer treatment (alongside surgery, radiotherapy and chemotherapy). For some aggressive cancers, such as advanced non-small-cell lung carcinoma, combination immunotherapies have resulted in unprecedented treatment efficacy for responding patients, and have become frontline therapies. Individualized immunotherapy, enabled by the identification of patient-specific mutations, neoantigens and biomarkers, and facilitated by advances in genomics and proteomics, promises to broaden the responder patient population. In this Perspective, we give an overview of immunotherapies leveraging engineering approaches, including the design of biomaterials, delivery strategies and nanotechnology solutions, for the realization of individualized cancer treatments such as nanoparticle vaccines customized with neoantigens, cell therapies based on patient-derived dendritic cells and T cells, and combinations of theranostic strategies. Developments in precision cancer immunotherapy will increasingly rely on the adoption of engineering principles.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
- R21 NS107894/NS/NINDS NIH HHS/United States
- U01 CA224160/CA/NCI NIH HHS/United States
- R01 NS105556/NS/NINDS NIH HHS/United States
- T32 GM007767/GM/NIGMS NIH HHS/United States
- R01 NS044556/NS/NINDS NIH HHS/United States
- R01 EB022563/EB/NIBIB NIH HHS/United States
- R01 AI127070/AI/NIAID NIH HHS/United States
- R01 CA210273/CA/NCI NIH HHS/United States
- R01 HL134569/HL/NHLBI NIH HHS/United States
- U01 CA210152/CA/NCI NIH HHS/United States
- R37 NS094804/NS/NINDS NIH HHS/United States
- R01 NS096756/NS/NINDS NIH HHS/United States
- R01 CA223804/CA/NCI NIH HHS/United States
- R21 NS091555/NS/NINDS NIH HHS/United States
- T32 DE007057/DE/NIDCR NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
