

Head Rules Over the Heart: Cardiac Manifestations of Cerebral Disorders
- PMID: 31406441
- PMCID: PMC6686577
- DOI: 10.5005/jp-journals-10071-23208
Head Rules Over the Heart: Cardiac Manifestations of Cerebral Disorders
Abstract
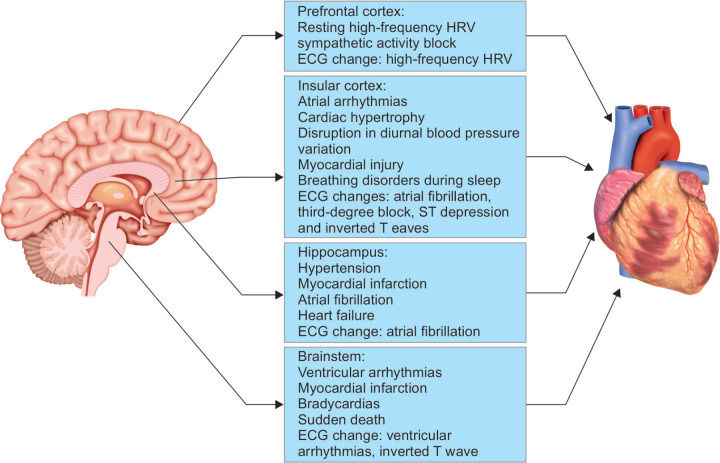
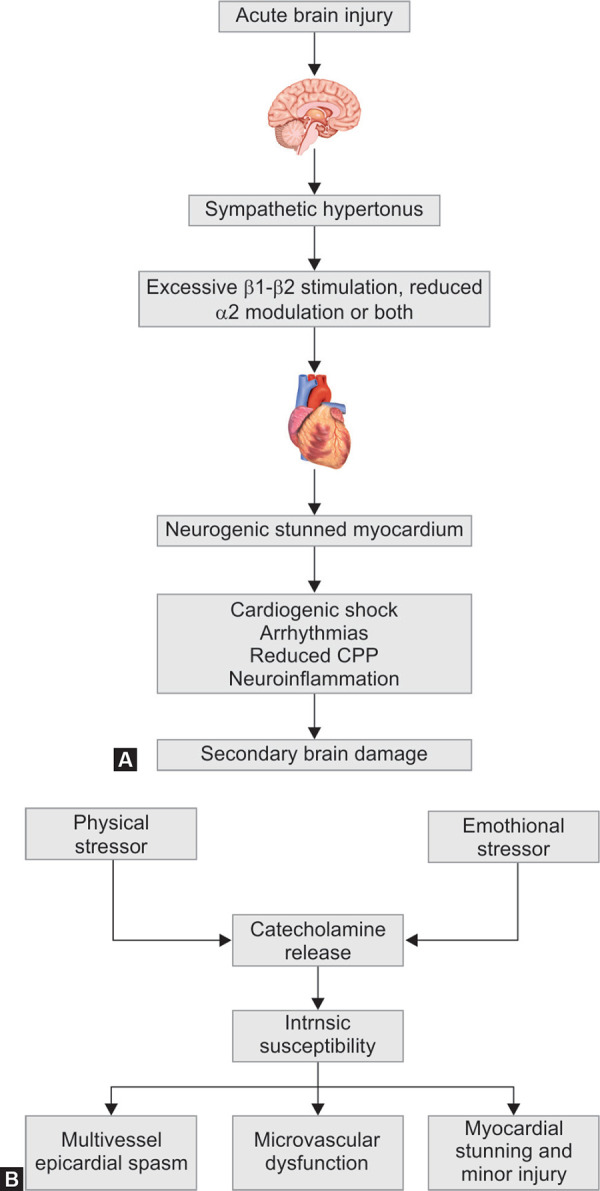
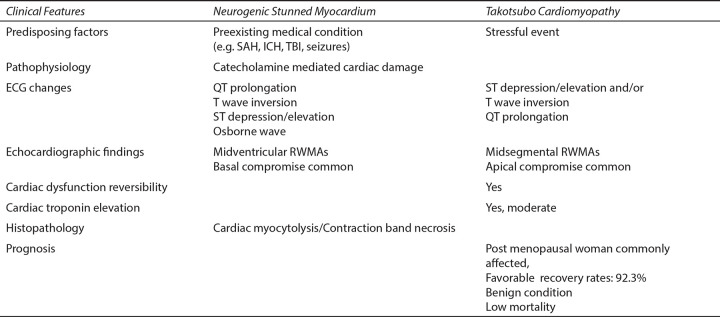
The Brain-Heart interaction is becoming increasingly important as the underlying pathophysiological mechanisms become better understood. "Neurocardiology" is a new field which explores the pathophysiological interplay of the brain and cardiovascular systems. Brain-heart cross-talk presents as a result of direct stimulation of some areas of the brain, leading to a sympathetic or parasympathetic response or it may present as a result of a neuroendocrine response attributing to a clinical picture of a sympathetic storm. It manifests as cardiac rhythm disturbances, hemodynamic perturbations and in the worst scenarios as cardiac failure and death. Brain-Heart interaction (BHI) is most commonly encountered in traumatic brain injury and subarachnoid hemorrhage presenting as dramatic electrocardiographic changes, neurogenic stunned myocardium or even as ventricular fibrillation. A well-known example of BHI is the panic disorders and emotional stress resulting in Tako-tsubo syndrome giving rise to supraventricular and ventricular tachycardias and transient left ventricular dysfunction. In this review article, we will discuss cardiovascular changes caused due to the disorders of specific brain regions such as the insular cortex, brainstem, prefrontal cortex, hippocampus and the hypothalamus; neuro-cardiac reflexes namely the Cushing's reflex, the Trigemino-cardiac reflex and the Vagal reflex; and other pathological states such as neurogenic stunned myocardium /Takotsubo cardiomyopathy. There is a growing interest among intensivists and anesthesiologists in brain heart interactions as there are an increasing number of cases being reported and there is a need to address unanswered questions, such as the incidence of these interactions, the multifactorial pathogenesis, individual susceptibility, the role of medications, and optimal management.
Key messages: BHI contribute in a significant way to the morbidity and mortality of neurological conditions such as traumatic brain injury, subarachnoid hemorrhage, cerebral infarction and status epilepticus. Constant vigilance and a high index of suspicion have to be exercised by clinicians to avoid misdiagnosis or delayed recognition. The entire clinical team involved in patient care should be aware of brain heart interaction to recognize these potentially life-threatening scenarios.
How to cite this article: Hrishi AP, Lionel KR, Prathapadas U. Head Rules Over the Heart: Cardiac Manifestations of Cerebral Disorders. Indian J Crit Care Med 2019;23(7):329-335.
Keywords: Neurocardiac axis; Neurocardiology; Neurological disorders.
Conflict of interest statement
Source of support: Nil Conflict of interest: None
Figures

References
-
- Natelson BH. Neurocardiology: an Interdisciplinary Area for the 80s. Archives Neurol. 1985;;42((2):):178-–184.. - PubMed
-
- Van der wall EE. The brain-heart connection; a round trip. Neth Heart J. 2011;;19::269-–270..
-
- Kukla P,, Jastrzebski M,, Praefort W. J-wave-associated ventricular fibrillation in a patient with a subarachnoid haemorrhage. Europace. 2012;;14::1063-–1064.. - PubMed
-
- Van der Wall EE. A broken heart: repair needed? Neth Heart J. 2012;;20::1-–2..
Publication types
LinkOut - more resources
Full Text Sources