

Mechanisms for hemodynamic instability related to renal replacement therapy: a narrative review
- PMID: 31407042
- PMCID: PMC6773820
- DOI: 10.1007/s00134-019-05707-w
Mechanisms for hemodynamic instability related to renal replacement therapy: a narrative review
Abstract
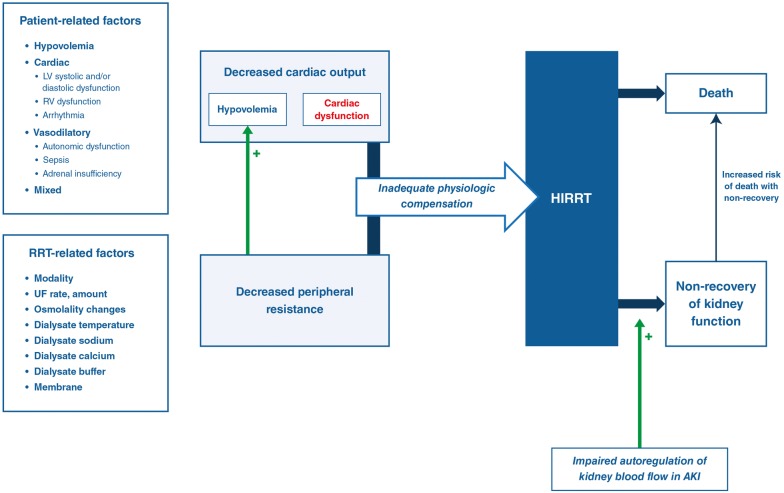
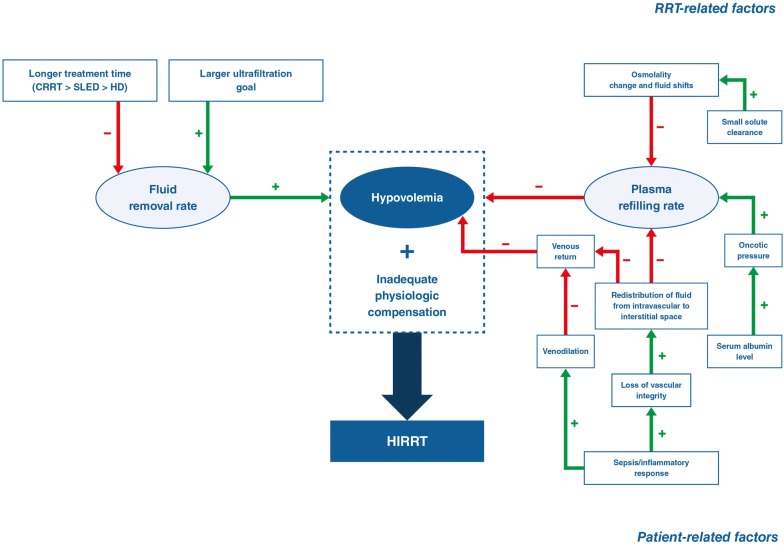
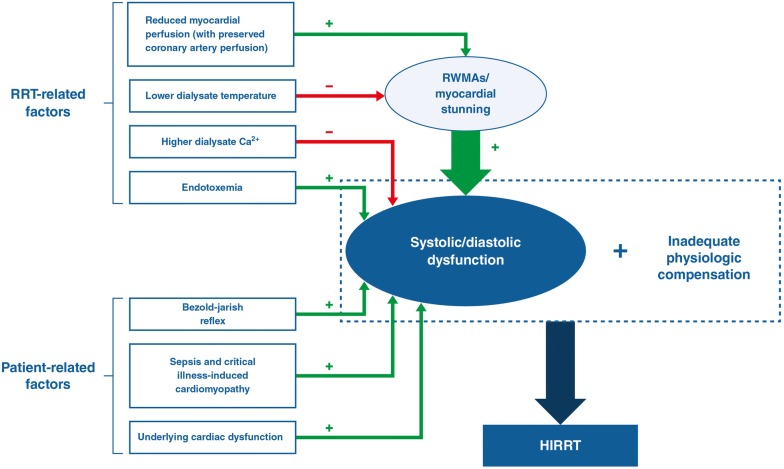
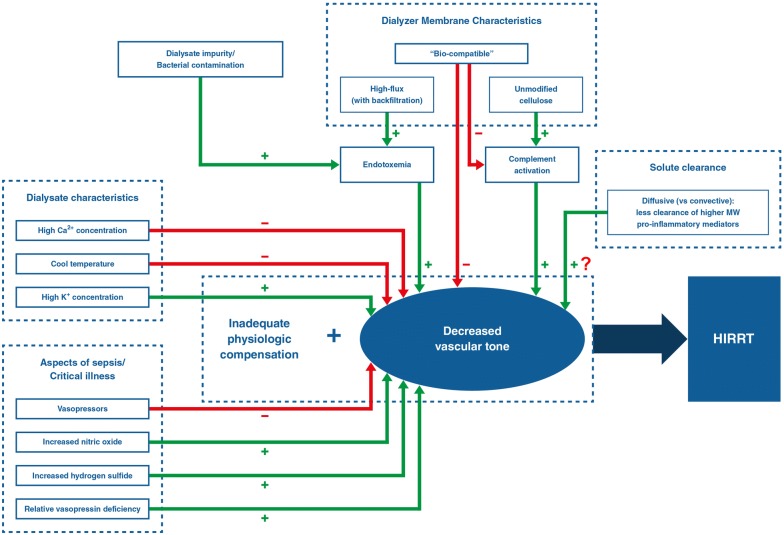
Hemodynamic instability related to renal replacement therapy (HIRRT) is a frequent complication of all renal replacement therapy (RRT) modalities commonly used in the intensive care unit. HIRRT is associated with increased mortality and may impair kidney recovery. Our current understanding of the physiologic basis for HIRRT comes primarily from studies of end-stage kidney disease patients on maintenance hemodialysis in whom HIRRT is referred to as 'intradialytic hypotension'. Nonetheless, there are many studies that provide additional insights into the underlying mechanisms for HIRRT specifically in critically ill patients. In particular, recent evidence challenges the notion that HIRRT is almost entirely related to excessive ultrafiltration. Although excessive ultrafiltration is a key mechanism, multiple other RRT-related mechanisms may precipitate HIRRT and this could have implications for how HIRRT should be managed (e.g., the appropriate response might not always be to reduce ultrafiltration, particularly in the context of significant fluid overload). This review briefly summarizes the incidence and adverse effects of HIRRT and reviews what is currently known regarding the mechanisms underpinning it. This includes consideration of the evidence that exists for various RRT-related interventions to prevent or limit HIRRT. An enhanced understanding of the mechanisms that underlie HIRRT, beyond just excessive ultrafiltration, may lead to more effective RRT-related interventions to mitigate its occurrence and consequences.
Keywords: Acute kidney injury; Blood pressure; Dialysis; Hemodynamic instability; Hypotension; Intradialytic hypotension; Renal replacement therapy.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures
References
-
- Hoste EA, Bagshaw SM, Bellomo R, Cely CM, Colman R, Cruz DN, Edipidis K, Forni LG, Gomersall CD, Govil D, Honore PM, Joannes-Boyau O, Joannidis M, Korhonen AM, Lavrentieva A, Mehta RL, Palevsky P, Roessler E, Ronco C, Uchino S, Vazquez JA, Vidal Andrade E, Webb S, Kellum JA. Epidemiology of acute kidney injury in critically ill patients: the multinational AKI-EPI study. Intensive Care Med. 2015;41:1411–1423. - PubMed
-
- Tonelli M, Astephen P, Andreou P, Beed S, Lundrigan P, Jindal K. Blood volume monitoring in intermittent hemodialysis for acute renal failure. Kidney Int. 2002;62:1075–1080. - PubMed
-
- Tanguay TA, Jensen L, Johnston C. Predicting episodes of hypotension by continuous blood volume monitoring among critically ill patients in acute renal failure on intermittent hemodialysis. CACCN. 2007;18:19–24. - PubMed
-
- Schortgen F, Soubrier N, Delclaux C, Thuong M, Girou E, Brun-Buisson C, Lemaire F, Brochard L. Hemodynamic tolerance of intermittent hemodialysis in critically ill patients: usefulness of practice guidelines. Am J Respir Crit Care Med. 2000;162:197–202. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
