

Isolation and Characterization of a Human Fetal Mesenchymal Stem Cell Population: Exploring the Potential for Cell Banking in Wound Healing Therapies
- PMID: 31407589
- PMCID: PMC6802149
- DOI: 10.1177/0963689718817524
Isolation and Characterization of a Human Fetal Mesenchymal Stem Cell Population: Exploring the Potential for Cell Banking in Wound Healing Therapies
Abstract
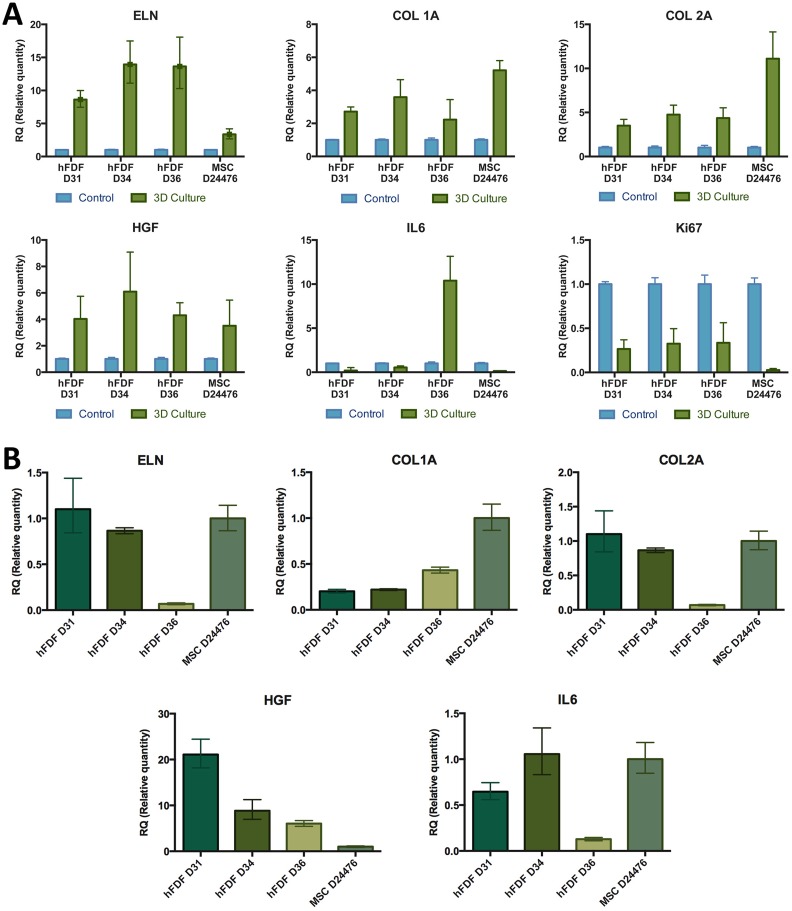
Various cell-based therapies are in development to address chronic and acute skin wound healing, for example for burns and trauma patients. An off-the-shelf source of allogeneic dermal cells could be beneficial for innovative therapies accelerating the healing in extensive wounds where the availability of a patient's own cells is limited. Human fetal-derived dermal fibroblasts (hFDFs) show high in vitro division rates, exhibit low immunological rejection properties, and present scarless wound healing in the fetus, and previous studies on human fetal tissue-derived cell therapies have shown promising results on tissue repair. However, little is known about cell lineage stability and cell differentiation during the cell expansion process, required for any potential therapeutic use. We describe an isolation method, characterize a population, and investigate its potential for cell banking and thus suitability as a potential product for cell grafting therapies. Our results show hFDFs and a bone marrow-derived mesenchymal stem cell (BM-MSC) line shared identification markers and in vitro multilineage differentiation potential into osteogenic, chondrogenic, and adipogenic lineages. The hFDF population exhibited similar cell characteristics as BM-MSCs while producing lower pro-inflammatory cytokine IL-6 levels and higher levels of the wound healing factor hepatocyte growth factor. We demonstrate in vitro differentiation of hFDFs, which may be a problem in maintaining long-term lineage stability, potentially limiting their use for cell banking and therapy development.
Keywords: cell banking; cell therapy; fetal-derived MSC; mesenchymal stem cells; wound healing.
Conflict of interest statement
Figures





Similar articles
-
In vitro characterization of human hair follicle dermal sheath mesenchymal stromal cells and their potential in enhancing diabetic wound healing.Cytotherapy. 2015 Aug;17(8):1036-51. doi: 10.1016/j.jcyt.2015.04.001. Epub 2015 May 13. Cytotherapy. 2015. PMID: 25981558
-
Tissue source determines the differentiation potentials of mesenchymal stem cells: a comparative study of human mesenchymal stem cells from bone marrow and adipose tissue.Stem Cell Res Ther. 2017 Dec 6;8(1):275. doi: 10.1186/s13287-017-0716-x. Stem Cell Res Ther. 2017. PMID: 29208029 Free PMC article.
-
Human amniotic mesenchymal stem cells and their paracrine factors promote wound healing by inhibiting heat stress-induced skin cell apoptosis and enhancing their proliferation through activating PI3K/AKT signaling pathway.Stem Cell Res Ther. 2019 Aug 9;10(1):247. doi: 10.1186/s13287-019-1366-y. Stem Cell Res Ther. 2019. PMID: 31399039 Free PMC article.
-
Concise review: role of mesenchymal stem cells in wound repair.Stem Cells Transl Med. 2012 Feb;1(2):142-9. doi: 10.5966/sctm.2011-0018. Stem Cells Transl Med. 2012. PMID: 23197761 Free PMC article. Review.
-
Immunomodulatory Effect of Cytokines in the Differentiation of Mesenchymal Stem Cells: A Review.Curr Stem Cell Res Ther. 2017;12(3):197-206. doi: 10.2174/1574888X11666160614103404. Curr Stem Cell Res Ther. 2017. PMID: 27306400 Review.
Cited by
-
Bicomponent Cutaneous Cell Therapy for Early Burn Care: Manufacturing Homogeneity and Epidermis-Structuring Functions of Clinical Grade FE002-SK2 Allogeneic Dermal Progenitor Fibroblasts.Pharmaceutics. 2025 May 24;17(6):692. doi: 10.3390/pharmaceutics17060692. Pharmaceutics. 2025. PMID: 40574004 Free PMC article.
-
Fetal progenitor cells for treatment of chronic limb ischemia.Am J Stem Cells. 2024 Jun 15;13(3):169-190. doi: 10.62347/MZKI8393. eCollection 2024. Am J Stem Cells. 2024. PMID: 39021376 Free PMC article.
-
Application of Mesenchymal Stem Cells and Exosome alone or Combination Therapy as a Treatment Strategy for Wound Healing.Cell Biochem Biophys. 2024 Dec;82(4):3209-3222. doi: 10.1007/s12013-024-01448-w. Epub 2024 Jul 28. Cell Biochem Biophys. 2024. PMID: 39068609 Review.
-
Holistic Approach of Swiss Fetal Progenitor Cell Banking: Optimizing Safe and Sustainable Substrates for Regenerative Medicine and Biotechnology.Front Bioeng Biotechnol. 2020 Oct 23;8:557758. doi: 10.3389/fbioe.2020.557758. eCollection 2020. Front Bioeng Biotechnol. 2020. PMID: 33195124 Free PMC article.
-
Retrospective Evaluation of Progenitor Biological Bandage Use: A Complementary and Safe Therapeutic Management Option for Prevention of Hypertrophic Scarring in Pediatric Burn Care.Pharmaceuticals (Basel). 2021 Feb 28;14(3):201. doi: 10.3390/ph14030201. Pharmaceuticals (Basel). 2021. PMID: 33671009 Free PMC article.
References
-
- National hospital ambulatory medical care survey: 2011 emergency department summary. 2011. [accessed July 7] http://www.cdc.gov/nchs/ahcd/web_tables.htm#2011.
-
- Argenta LC, Morykwas MJ. Vacuum-assisted closure: a new method for wound control and treatment: clinical experience. Ann Plast Surg. 1997;38(6):563–577. - PubMed
-
- Balakrishnan C, Hashim M, Gao D. The effect of partial-thickness facial burns on social functioning. J Burn Care Rehabil. 1999;20(3):224–225. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
