

Molecular Testing Versus Diagnostic Lobectomy in Bethesda III/IV Thyroid Nodules: A Cost-Effectiveness Analysis
- PMID: 31407625
- PMCID: PMC7366255
- DOI: 10.1089/thy.2018.0779
Molecular Testing Versus Diagnostic Lobectomy in Bethesda III/IV Thyroid Nodules: A Cost-Effectiveness Analysis
Abstract
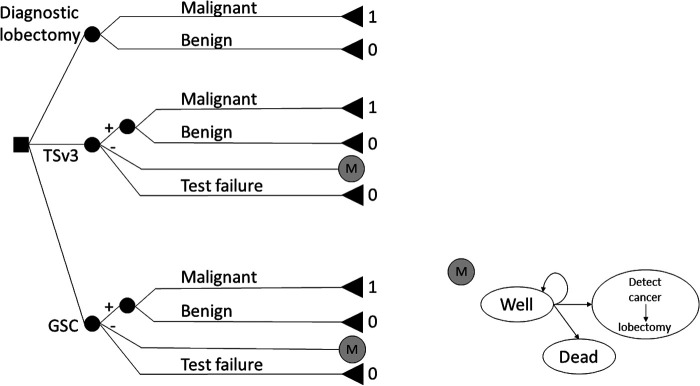
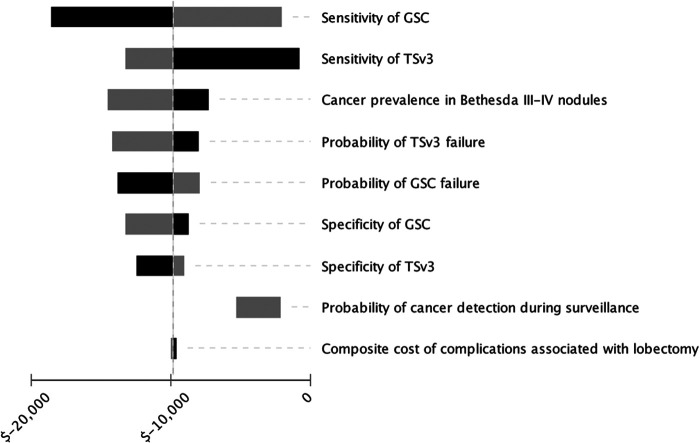
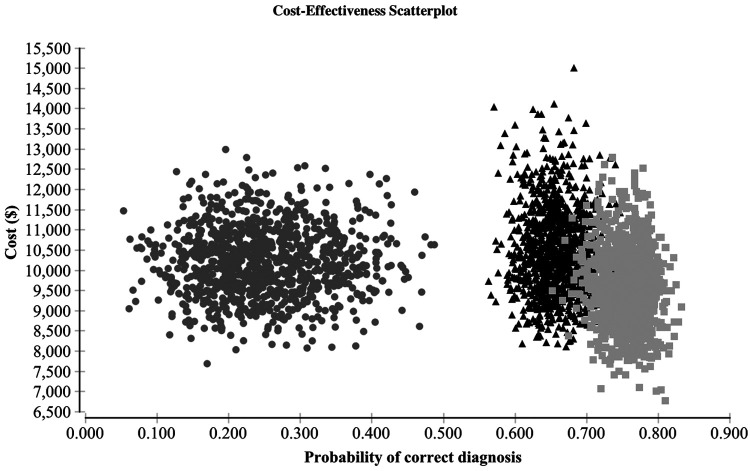
Background: Molecular tests (MT) using gene expression and/or mutational analysis have been developed to reduce the need for diagnostic surgery for indeterminate (Bethesda III/IV) thyroid nodules. Prior cost-effectiveness studies have shown mixed results but none has included the recent and more comprehensive versions of the two commonly utilized MT. The aim of this study is to compare the cost-effectiveness of diagnostic lobectomy (DL), the Afirma Gene Sequencing Classifier (GSC), and ThyroSeq version 3 (TSv3). Methods: A decision tree from the payer perspective was created using a base case of a 40-year-old euthyroid woman with a solitary 2 cm Bethesda III or IV thyroid nodule. In this model, all patients in the DL arm had lobectomy, which was also performed for patients with positive MT, while those with negative MT underwent 20 years of surveillance. The outcome was a correct diagnosis, defined as malignant histology after DL or 20 years of nodule stability after negative MT. Costs were obtained from the Centers for Medicare & Medicaid Services (CMS) data and existing literature, and probabilities were obtained from the literature. Sensitivity analysis was performed for costs, pretest probability of malignancy, and performance parameters. Results: The cost per correct diagnosis was $14,277 for TSv3, $17,873 for GSC, and $38,408 for DL. TSv3 was preferred over both GSC and DL. One-way sensitivity analysis between TSv3 and GSC demonstrated that the results were robust to variations in cost, cancer prevalence, and length of surveillance. In the two-way sensitivity analysis, TSv3 was preferred over GSC at all considered test costs, and in probabilistic sensitivity analysis, TSv3 was the preferred management strategy in 68.5% of cases. Conclusions: In hypothetical modeling to determine whether surgery versus MT is optimal for indeterminate (Bethesda III/IV) nodules, either of the major MT was considerably more cost-effective than DL, although TSv3 was more likely to be cost-effective than GSC. Use of either MT adjunct should be strongly considered in the absence of other indications for thyroidectomy.
Keywords: Bethesda III/IV nodule; cost-effectiveness; diagnostic lobectomy; molecular testing; thyroid nodule.
Conflict of interest statement
The authors have no commercial affiliation associated with this article. Some of the authors (M.S.R., K.L.M., S.E.C., and L.Y.) are employees of the University of Pittsburgh Physicians, which is an affiliate of UPMC. UPMC has granted CBLPath, Inc. a license to market the ThyroSeq trademark for commercial use. The authors receive no direct or indirect compensation related to CBLPath, Inc.
Figures
References
-
- Bongiovanni M, Spitale A, Faquin WC, Mazzucchelli L, Baloch ZW. 2012. The Bethesda System for Reporting Thyroid Cytopathology: a meta-analysis. Acta Cytol 56:333–339 - PubMed
-
- Cooper DS, Doherty GM, Haugen BR, Kloos RT, Lee SL, Mandel SJ, Mazzaferri EL, McIver B, Pacini F, Schlumberger M, Sherman SI, Steward DL, Tuttle RM. 2006. Revised American Thyroid Association management guidelines for patients with thyroid nodules and differentiated thyroid cancer. Thyroid 19:1167–1219 - PubMed
-
- Cooper DS, Doherty GM, Haugen BR, Kloos RT, Lee SL, Mandel SJ, Mazzaferri EL, McIver B, Pacini F, Schlumberger M, Sherman SI, Steward DL, Tuttle RM. 2009. Revised American Thyroid Association management guidelines for patients with thyroid nodules and differentiated thyroid cancer: the American Thyroid Association (ATA) Guidelines Taskforce on Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid 19:1167–1214 - PubMed
-
- Sosa JA, Hanna JW, Robinson KA, Lanman RB. 2013. Increases in thyroid nodule fine-needle aspirations, operations, and diagnoses of thyroid cancer in the United States. Surgery 154:1420–1426; discussion 1426–1427. - PubMed
-
- Nikiforov YE. 2017. Role of molecular markers in thyroid nodule management: then and now. Endocr Pract 23:979–988 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
