

Mortality Risk of Nonoperative Papillary Thyroid Carcinoma: A Corollary for Active Surveillance
- PMID: 31407637
- PMCID: PMC7476400
- DOI: 10.1089/thy.2019.0060
Mortality Risk of Nonoperative Papillary Thyroid Carcinoma: A Corollary for Active Surveillance
Abstract
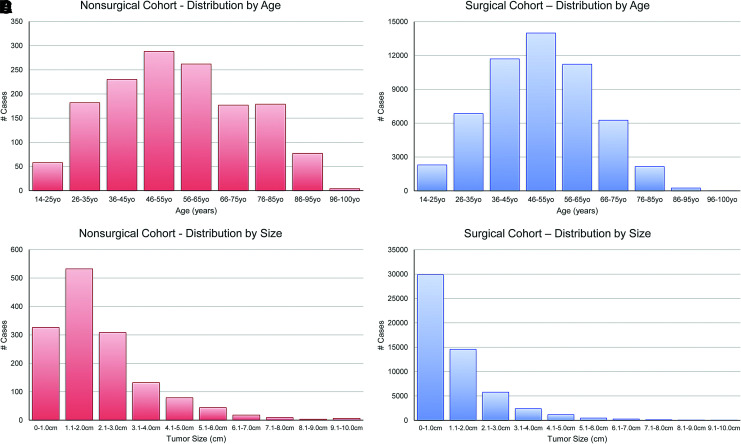
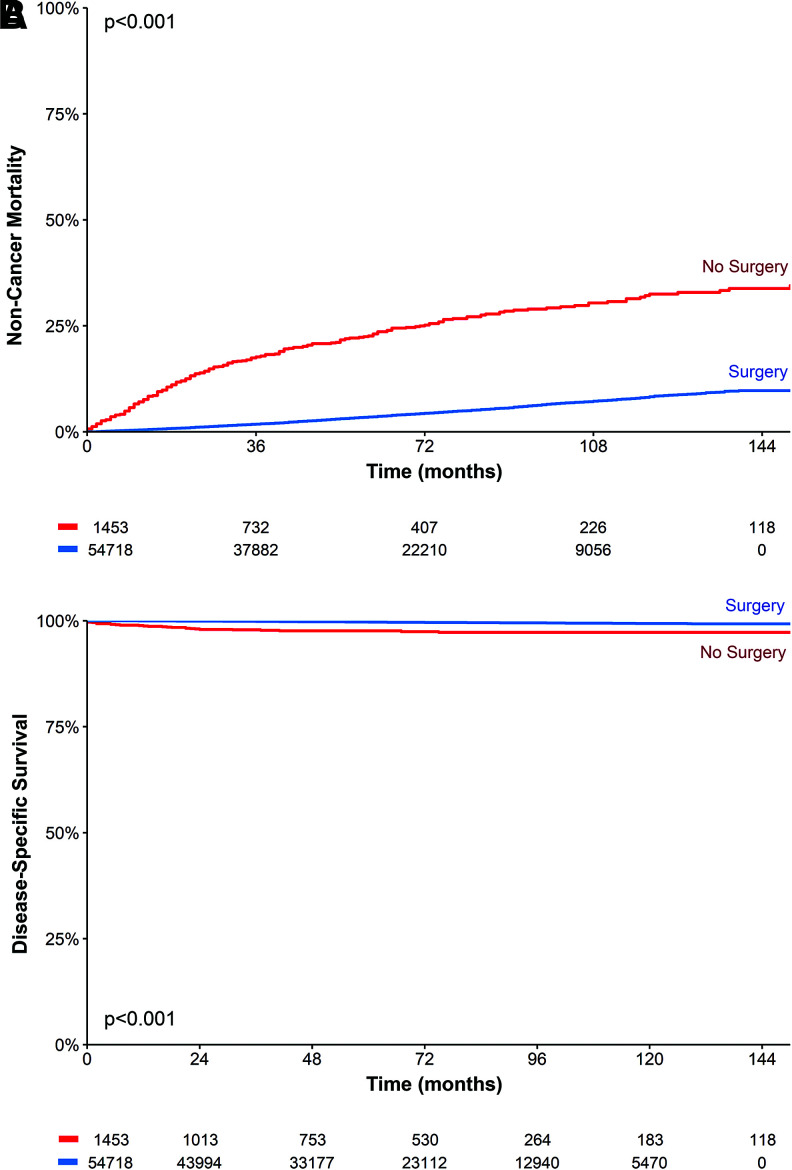
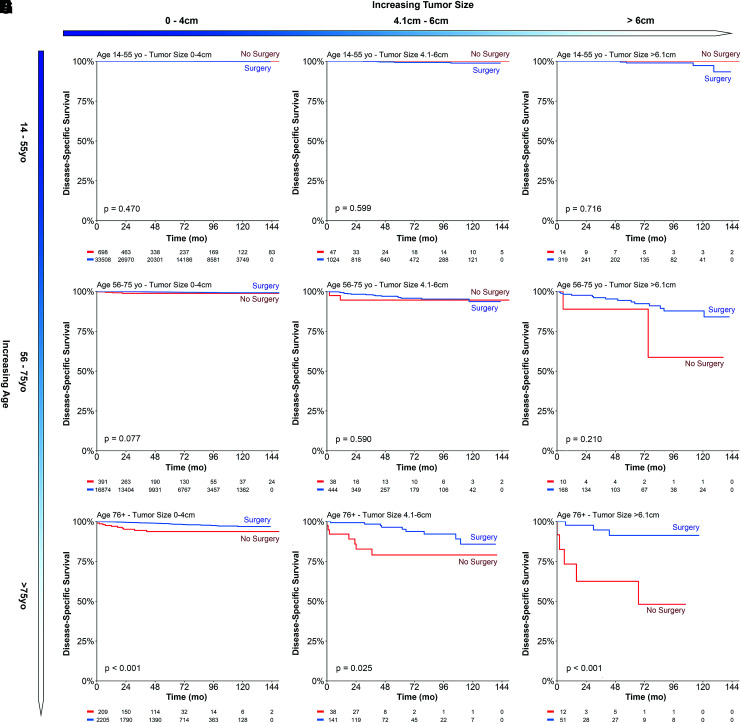
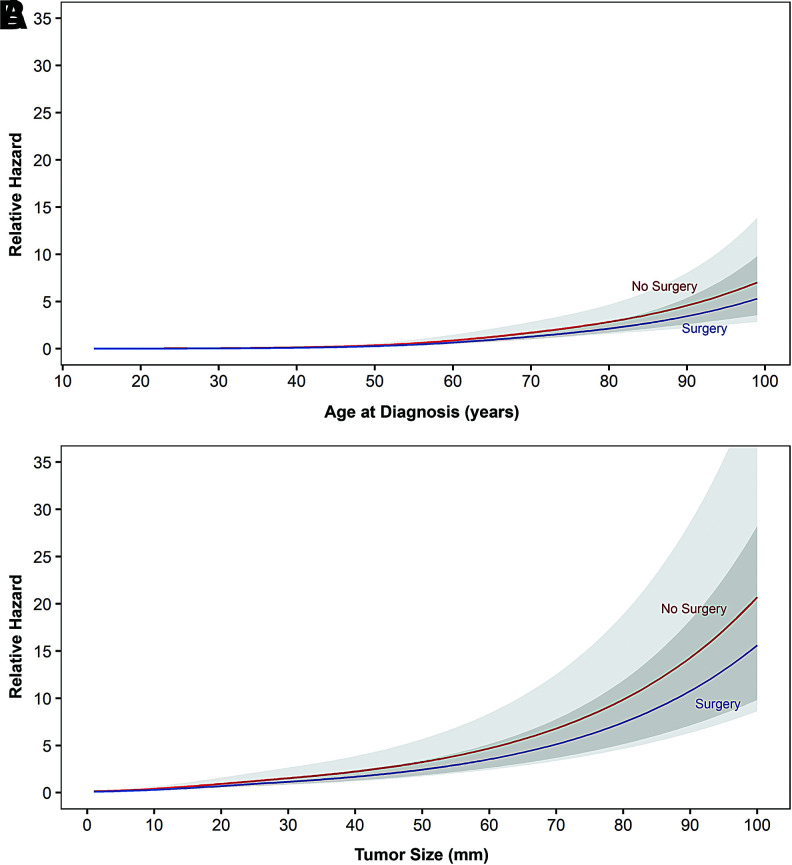
Background: Active surveillance is established as an alternative to surgery for papillary thyroid microcarcinomas, but inclusion criteria and mortality risk for pursuing a nonsurgical approach have not been clearly defined. To gauge the feasibility of expanding active surveillance thresholds, we investigated the effects of increasing size and age on disease-specific survival (DSS) in a large nonoperative thyroid cancer cohort, compared against a matched group of surgical patients. Methods: Papillary thyroid carcinoma patients staged T1-4N0M0 were identified in the Surveillance, Epidemiology, and End Results (SEER) database between 1975 and 2015, stratified by nonsurgical and surgical management. Propensity score matching was performed to adjust for imbalances in covariates. Multivariable models were constructed using restricted cubic splines to model nonlinear relationships of age and tumor size with DSS. Results: Overall, 1453 nonoperative patients and 54,718 surgical patients met the inclusion criteria. Collectively, increasing age and size after certain thresholds independently led to greater differences in DSS between nonsurgical and surgical patients. For younger ages (14-55 years), surgical approach compared with nonsurgical approach was not associated with any difference in the 10-year DSS among 0-4 cm cancers (99.8% vs. 100%, p = 0.470), 4.1-6 cm cancers (98.8% vs. 100%, p = 0.599), or >6 cm cancers (97.3% vs. 100%, p = 0.718). Older patients with larger tumors (>75 years, >6 cm) demonstrated the greatest difference in DSS (48.1% vs. 91.3%, p < 0.001). Similar results were found when applying propensity score matching. For age, restricted cubic spline plots showed minimal relative survival hazard in nonoperative cases beginning after age 60 years, with a change point illustrating acceleration in relative hazard beyond age 72 years. For size, relative survival hazard was observed after 2.0 cm and increased slowly with nodule growth up to an inflection point of 4.5 cm. Beyond this, mortality risk escalated with each additional year without plateau. Conclusions: Increasing age and size lead to progressively greater mortality risk without surgery, but only beyond certain thresholds. We define escalating gradients at which a nonsurgical approach may be deemed appropriate, and beyond which survival benefits from surgery become apparent. Such findings reconcile controversial observations regarding age and size in active surveillance and further reshape evolving treatment paradigms in thyroid cancer.
Keywords: active surveillance; low-risk cancer; nonsurgical treatment; papillary thyroid carcinoma; thyroid cancer.
Conflict of interest statement
Z.S.Z. was on the external advisory board for the Scripps Proton Therapy Center and has been a paid consultant for EMD Serono. For all other authors, no competing financial interests exist.
Figures
References
-
- Davies L, Welch HG. 2014. Current thyroid cancer trends in the United States. JAMA Otolaryngol Head Neck Surg 140:317–322 - PubMed
-
- US Preventive Services Task Force, Bibbins-Domingo K, Grossman DC, Curry SJ, Barry MJ, Davidson KW, Doubeni CA, Epling JW, Jr, Kemper AR, Krist AH, Kurth AE, Landefeld CS, Mangione CM, Phipps MG, Silverstein M, Simon MA, Siu AL, Tseng CW. 2017. Screening for thyroid cancer: US Preventive Services Task Force Recommendation Statement. JAMA 317:1882–1887 - PubMed
-
- Haugen BR, Alexander EK, Bible KC, Doherty GM, Mandel SJ, Nikiforov YE, Pacini F, Randolph GW, Sawka AM, Schlumberger M, Schuff KG, Sherman SI, Sosa JA, Steward DL, Tuttle RM, Wartofsky L. 2016. 2015 American Thyroid Association Management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer: the American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid 26:1–133 - PMC - PubMed
-
- Ito Y, Miyauchi A, Inoue H, Fukushima M, Kihara M, Higashiyama T, Tomoda C, Takamura Y, Kobayashi K, Miya A. 2010. An observational trial for papillary thyroid microcarcinoma in Japanese patients. World J Surg 34:28–35 - PubMed
Publication types
MeSH terms
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
