

In Utero Amniotic Fluid Stem Cell Therapy Protects Against Myelomeningocele via Spinal Cord Coverage and Hepatocyte Growth Factor Secretion
- PMID: 31407874
- PMCID: PMC6811697
- DOI: 10.1002/sctm.19-0002
In Utero Amniotic Fluid Stem Cell Therapy Protects Against Myelomeningocele via Spinal Cord Coverage and Hepatocyte Growth Factor Secretion
Abstract
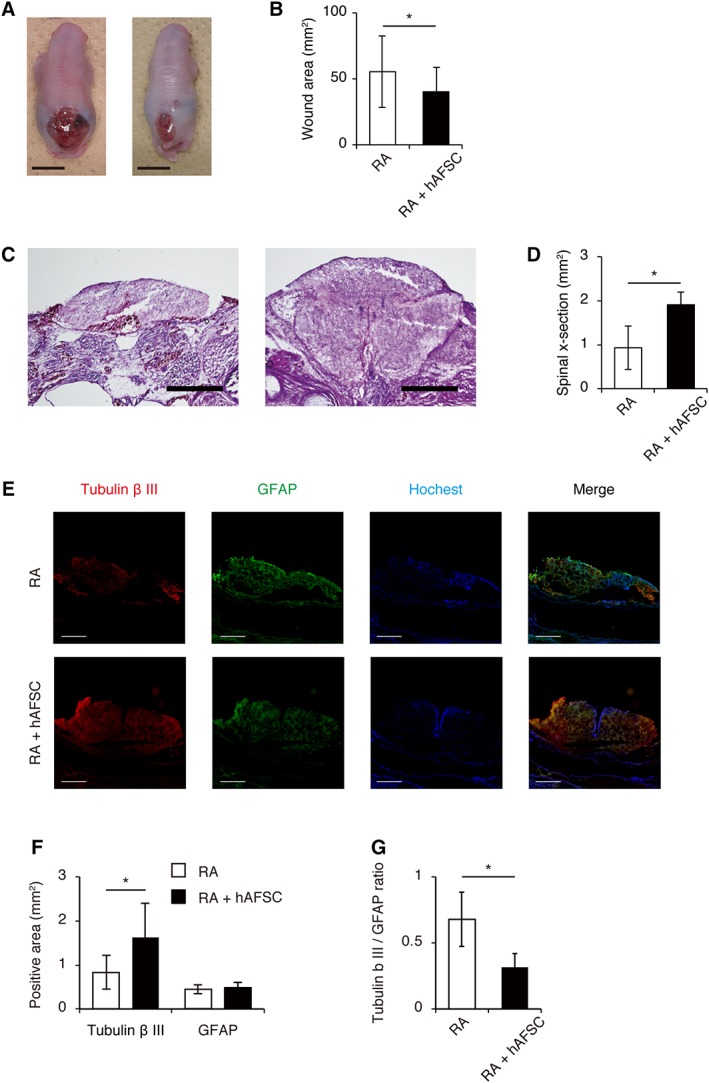
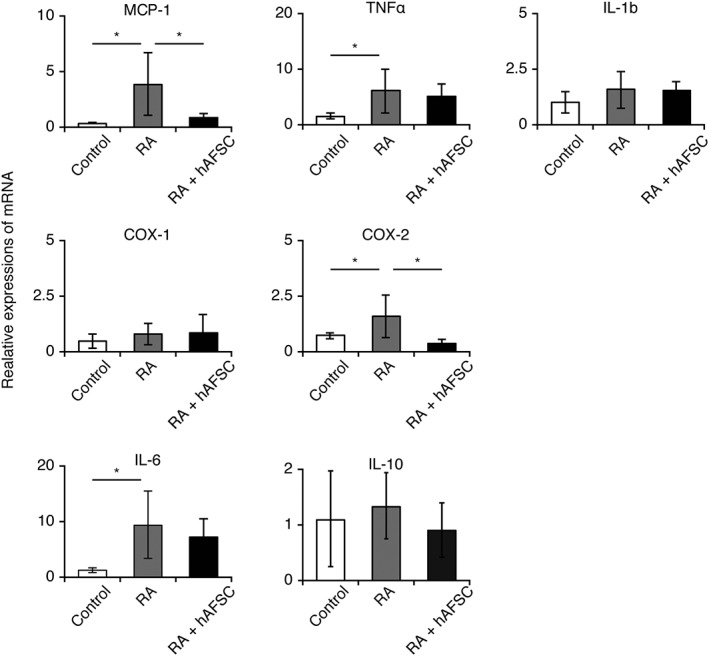
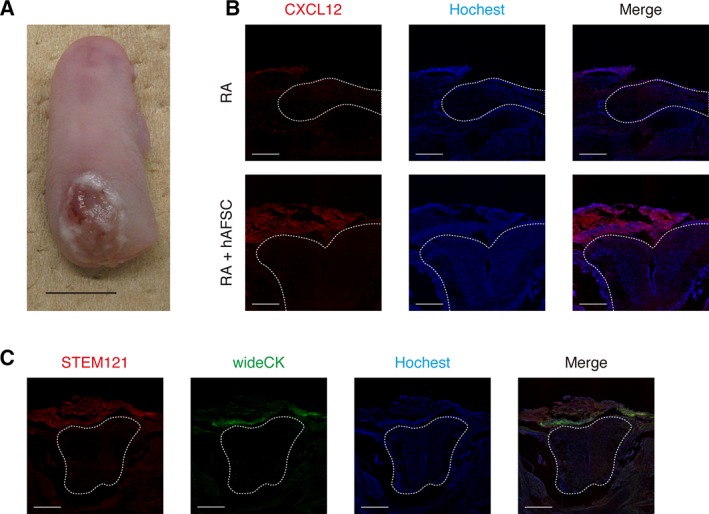
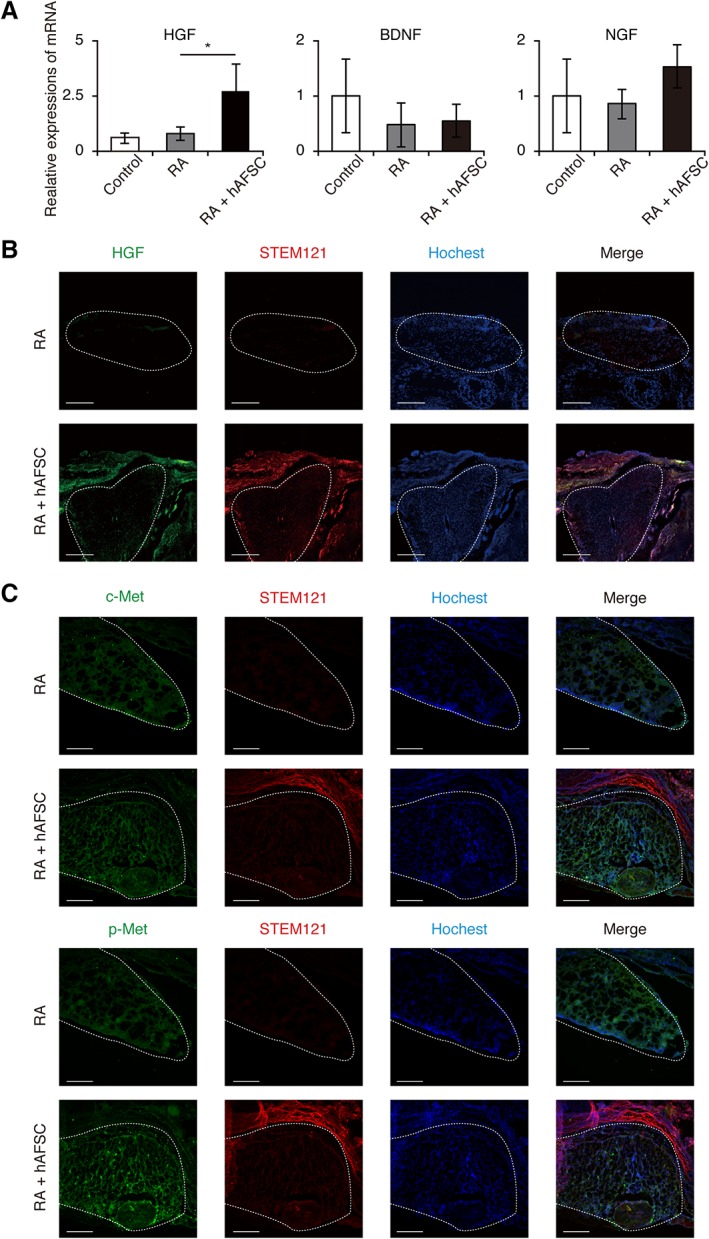
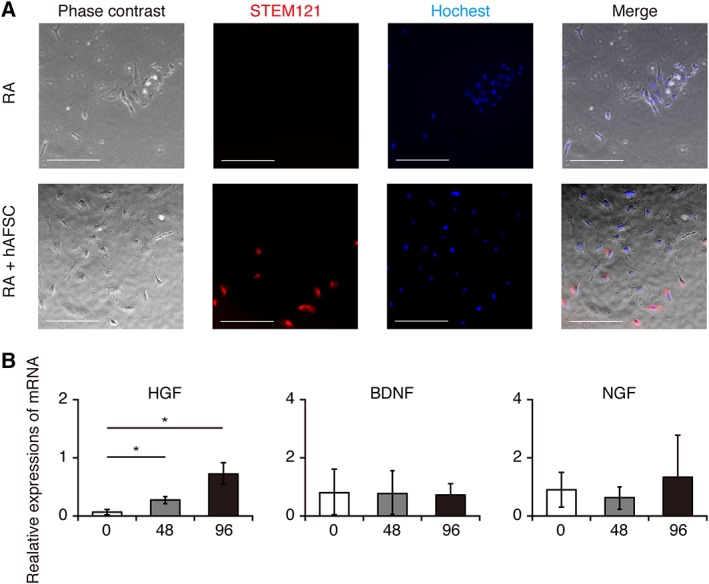
Despite the poor prognosis associated with myelomeningocele (MMC), the options for prenatal treatments are still limited. Recently, fetal cellular therapy has become a new option for treating birth defects, although the therapeutic effects and mechanisms associated with such treatments remain unclear. The use of human amniotic fluid stem cells (hAFSCs) is ideal with respect to immunoreactivity and cell propagation. The prenatal diagnosis of MMC during early stages of pregnancy could allow for the ex vivo proliferation and modulation of autologous hAFSCs for use in utero stem cell therapy. Therefore, we investigated the therapeutic effects and mechanisms of hAFSCs-based treatment for fetal MMC. hAFSCs were isolated as CD117-positive cells from the amniotic fluid of 15- to 17-week pregnant women who underwent amniocentesis for prenatal diagnosis and consented to this study. Rat dams were exposed to retinoic acid to induce fetal MMC and were subsequently injected with hAFSCs in each amniotic cavity. We measured the exposed area of the spinal cord and hepatocyte growth factor (HGF) levels at the lesion. The exposed spinal area of the hAFSC-treated group was significantly smaller than that of the control group. Immunohistochemical analysis demonstrated a reduction in neuronal damage such as neurodegeneration and astrogliosis in the hAFSC-treated group. Additionally, in lesions of the hAFSC-treated group, HGF expression was upregulated and HGF-positive hAFSCs were identified, suggesting that these cells migrated to the lesion and secreted HGF to suppress neuronal damage and induce neurogenesis. Therefore, in utero hAFSC therapy could become a novel strategy for fetal MMC. Stem Cells Translational Medicine 2019;8:1170-1179.
Keywords: Amniotic fluid stem cells; Fetal cellular therapy; Hepatocyte growth factor; Myelomeningocele; Spinal cord.
© 2019 The Authors. Stem Cells Translational Medicine published by Wiley Periodicals, Inc. on behalf of AlphaMed Press.
Conflict of interest statement
H.O. is a founding scientist and a paid Scientific Advisor of SanBio Co, Ltd. and K Pharma, Inc. The other authors indicated no potential conflicts of interest.
Figures
References
-
- Mitchell LE, Adzick NS, Melchionne J et al. Spina bifida. Lancet 2004;364:1885–1895. - PubMed
-
- Danzer E, Zhang L, Radu A et al. Amniotic fluid levels of glial fibrillary acidic protein in fetal rats with retinoic acid induced myelomeningocele: Apotential marker for spinal cord injury. Am J Obstet Gynecol 2011;204:178.e1–178.e11. - PubMed
-
- Dionigi B, Ahmed A, Brazzo J 3rd et al. Partial or complete coverage of experimental spina bifida by simple intra‐amniotic injection of concentrated amniotic mesenchymal stem cells. J Pediatr Surg 2015;50:69–73. - PubMed
-
- Dionigi B, Brazzo JA 3rd, Ahmed A et al. Trans‐amniotic stem cell therapy (TRASCET) minimizes Chiari‐II malformation in experimental spina bifida. J Pediatr Surg 2015;50:1037–1041. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
